- What Are Tactile Cues and How Do They Help Recovery? - 28 March 2026
- Parsonage-Turner Syndrome and COVID-19: What the Research Shows - 28 March 2026
- Managing Pain in the Acute Phase of Parsonage-Turner Syndrome - 28 March 2026
You might’ve heard the term “tactile cues” if you’ve spent any time looking into hypermobility rehab. It’s one of those phrases that gets thrown around a lot in our world, and for good reason, it’s central to how we work with people at The Fibro Guy. But what are tactile cues actually, and why do they seem to make such a difference? More importantly, how do they apply to nerve injury recovery, particularly for those with Parsonage-Turner syndrome?
This article is part of our comprehensive guide to Parsonage-Turner syndrome.
This article is going to break it all down. We’ll cover the science, the practical applications, and why we think tactile cues represent one of the most underused tools in rehabilitation. We’ve linked out to our complete PTS guide and our articles on brain changes after nerve injury and PTS exercise and rehabilitation if you want the broader picture. But this page is specifically about tactile cues, what they are, how they work, and how you can start using them.
What Are Tactile Cues?
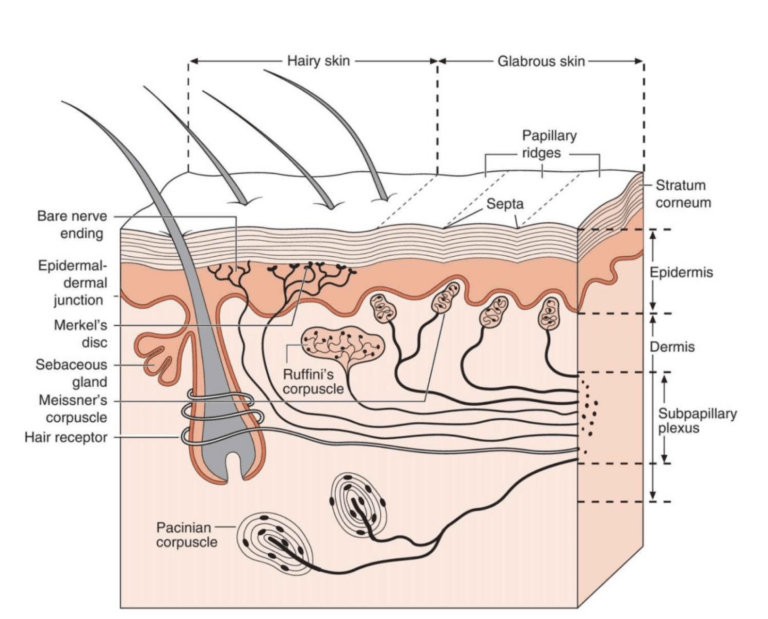
At their simplest, tactile cues are pieces of physical sensory input, things like touch, pressure, resistance, or texture, that give your brain clearer information about where a joint is and how it’s moving. But that description doesn’t quite capture it. This isn’t just about “touching” something. It’s strategic sensory feedback designed to change how your nervous system processes movement.
Think of it this way. Your brain builds maps of your body based on the sensory information it receives. These maps, stored in the somatosensory cortex, determine how accurately your brain knows where each body part is in space, from your elbows to your wrists to your shoulder blades. When the sensory input is clear and consistent, the maps are detailed and precise. When it’s not, the maps become blurry. And blurry maps mean imprecise movement control [1].
Tactile cues work by adding extra sensory information to sharpen those maps. A resistance band wrapped around the trunk during a shoulder exercise isn’t there for resistance in the traditional sense, it’s there because the pressure gives your brain additional data about where your ribcage is relative to your shoulder blade. A strip of KT tape isn’t just “support”, it’s a constant stream of sensory input telling the brain where that joint is.
We’ve been using tactile cues with those with hypermobility for years, and the results speak for themselves. But the science behind why they work is genuinely fascinating, and it applies to far more than just hypermobility.
The Science Behind Tactile Cues
So why does adding external sensory input actually change how the brain controls movement? The answer lies in something called cortical mapping, and it’s one of the most important concepts when it comes to understanding rehabilitation.
Your somatosensory cortex contains a map of your entire body. You might have seen those odd-looking diagrams of a “homunculus”, a distorted human figure where the hands and face are enormous because they have the most sensory nerve endings. The size of each body part on that map corresponds to how much sensory input the brain receives from it. More input means a bigger, more detailed map. Less input means a smaller, fuzzier one.
Now here’s where it gets interesting. These maps aren’t fixed. They change based on experience, injury, and the quality of sensory information coming in. This is neuroplasticity in action. And it cuts both ways. If you lose sensory input from an area, say through nerve damage or through the poor proprioception that comes with hypermobility, the cortical map for that area shrinks and becomes less defined [2]. The brain essentially starts to “forget” the detailed layout of that body part.
However, the really exciting research shows that this process is reversible. A landmark study by Florence and colleagues in 2001 demonstrated that sensory enrichment, providing enhanced tactile stimulation to an area, can actually restore cortical maps after nerve injury [1]. They showed that the brain’s representation of a body part could be rebuilt by giving it richer sensory input. That’s not speculation, that’s measurable cortical change.
More recent work has reinforced this. Philip and Zink’s 2020 scoping review of cortical plasticity interventions for peripheral nerve injury identified several rehabilitation approaches based on this principle, including traditional sensory re-education, activity-based sensory re-education, and cross-modal sensory substitution [3]. All of these share a common thread: they work by providing the brain with enhanced sensory information to rebuild its internal maps.
When it comes to how we apply this practically, tactile cues are our primary tool for delivering that enhanced sensory input. They’re the bridge between the laboratory research on cortical plasticity and what actually happens in a rehab session.
Why Tactile Cues Matter for Those With Hypermobility
If you’ve got hypermobility or EDS, there’s a good chance your proprioception isn’t great. This is well documented in the research. Proprioception, your body’s ability to sense where it is in space without looking, relies on receptors in your joints, muscles and tendons. When those joints move further than expected, or when the connective tissue is laxer than typical, the signals those receptors send become less reliable [4].
We often describe this to our clients using a map analogy. Imagine trying to navigate a city using a really low-resolution map. You can see the rough layout, maybe the main roads, but you can’t see the side streets, the landmarks, or the details that would help you move around accurately. That’s what proprioception is like for a lot of those with hypermobility. The brain has a general idea of where the joint is, but the resolution is too low for precise control.
And what happens when the brain can’t precisely control a joint? It compensates. You get muscle guarding, co-contraction, fear of movement, and those compensatory patterns that so many of our clients recognise, things like rib subluxations from altered shoulder mechanics or postural adaptations that develop over time. The anxiety that often accompanies hypermobility isn’t separate from the proprioceptive problem, it’s partly driven by it. When your brain doesn’t trust the information it’s getting about where your body is, it ramps up the threat response.
So tactile cues increase the resolution of that map. By adding external sensory input, pressure from a band, feedback from tape, contact with a textured surface, you’re giving the brain more data points. It’s like upgrading from a blurry map to a detailed one. And when the brain has a clearer picture of where a joint is, it can control it more effectively.
This is why we use tactile cues for everything from core stability work to shoulder blade rehabilitation to lower limb motor control. The principle is the same regardless of the body part: give the brain better information and it produces better movement output.
Side note, and this is something I find genuinely interesting. We’ve noticed over the years that tactile cues seem to work almost immediately for some people. Not in terms of structural change obviously, that takes time, but in terms of movement quality. Someone who’s been struggling with a particular movement will put a band on and suddenly the movement cleans up. It’s as if the brain was always capable of producing the movement, it just didn’t have enough information to do it confidently. Whether that’s a proprioceptive thing or a confidence thing or both, I’m not sure, but it’s something we see again and again.
Tactile Cues for Nerve Injury Recovery
Now, this is where things get particularly relevant for anyone recovering from a nerve injury like Parsonage-Turner syndrome. And the reason is that nerve injury creates an even more dramatic version of the same cortical mapping problem we just discussed.
When the brachial plexus is damaged in PTS, the sensory pathways between the arm and the brain are disrupted. The brain stops receiving reliable signals from the affected area. And just like we described with hypermobility, the cortical maps become disordered. But with nerve injury, it’s often more severe. A 2022 fMRI study by Lustenhouwer and colleagues found decreased cerebral activity in visuomotor areas of the brain in patients with neuralgic amyotrophy, and this directly correlated with persistent pain and dysfunction [2]. The worse the cortical changes, the more pain people experienced.
This is what’s called maladaptive plasticity. The brain adapts to the loss of input, but it adapts in ways that actually make things worse, somewhat similar to what we see with neurological processing issues in other conditions. The cortical map doesn’t just become blurry it becomes distorted. And this is why some people with PTS still have functional problems even after the nerve itself has regenerated. The peripheral hardware has been repaired, but the central software hasn’t been updated [5].
However, and this is the encouraging part, if tactile input can restore cortical maps after nerve injury (which Florence et al. demonstrated back in 2001), then there’s a clear rationale for using tactile cues during PTS recovery. You’re not just waiting for the nerve to regrow and hoping the brain figures it out. You’re actively feeding the brain sensory information to help it rebuild those maps as reinnervation happens.
The same principles we use for those with hypermobility apply directly to PTS rehabilitation, but arguably they matter even more. When it comes to nerve injuries, the cortical mapping problem is the thing that often determines long-term outcomes. Research on brachial plexus rehabilitation has specifically identified tactile interaction with different textures and temperatures as effective for sensory re-education, and mirror visual feedback has been shown to create stronger motor-sensory connections than classical rehab alone [6][7].
We cover the brain science in much more detail in our article on cortical changes after PTS, and the recovery phases article explains when tactile cues become most relevant in the rehabilitation timeline.
How to Use Tactile Cues in Practice
Right, so the science makes sense. But what does this actually look like in a rehab session? How do you use tactile cues practically?
Well, there are several approaches and the specific technique depends on what you’re trying to achieve and which body part you’re working with. Here are the main methods we use.
Resistance Bands for Proprioceptive Feedback
This is probably the most common way we use tactile cues. A light resistance band wrapped around the trunk or placed around a joint creates constant pressure feedback. For shoulder blade work, a band around the ribcage gives the brain a clear reference point for where the thorax is, making it much easier to control scapular movement. The band isn’t there to make the exercise harder. It’s there to make the movement clearer.
Taping for Sustained Input
When it comes to providing a constant tactile cue throughout the day, KT tape and similar taping methods are really useful. The tape sits on the skin and provides ongoing sensory feedback about joint position. It’s not providing structural support in any meaningful way, the adhesion simply isn’t strong enough for that, but it doesn’t need to. The sensory input is the point. For those recovering from PTS, taping the shoulder girdle area can provide that constant stream of proprioceptive information while the nerves are recovering. Compression garments work on a similar principle, providing broad area tactile feedback.
Unstable Surface Training
Using unstable surfaces like a slackline for upper body training is something we’ve had brilliant results with. The instability forces the brain to process far more sensory information than a stable surface would require, it massively increases the demands on the proprioceptive system, somewhat like how CO2 tolerance training pushes the respiratory system to adapt. For upper body work, this means the brain has to work much harder to map where the shoulder and arm are in space.
Manual Pressure and Guided Touch
In clinic, we use manual tactile cues a lot. Placing a hand on a specific muscle or joint while someone performs a movement helps the brain “tune in” to that area. It’s a bit like pointing at something on a map, you’re directing the brain’s attention to a specific body part. This is particularly useful in the early stages of PTS recovery when motor control is significantly compromised, or after an EDS flare-up when proprioception often dips. We talk about pain management approaches in the acute phase, but once someone moves into rehabilitation, manual tactile cues become a core part of the work.
Progressive Complexity
The key thing with tactile cues is progression. You start simple, a band around the trunk, some tape on the shoulder, basic movements with manual guidance. And over time you increase the complexity. The tactile cues become less overt as the brain’s maps improve, the movements become more challenging and you gradually reduce the external feedback as the internal systems take over. It’s not a replacement for exercise, it’s an enhancement that makes the exercise more effective.
For those with hypermobility who are also recovering from PTS, this progressive approach is especially important. You’re dealing with two layers of proprioceptive deficit, the baseline hypermobility-related reduction plus the nerve injury disruption. When it comes to PTS rehabilitation in this population, tactile cues aren’t optional, they’re essential.
What Tactile Cues Don’t Do
We should be honest here because there’s a risk of overselling this. Tactile cues are not a miracle fix. They don’t heal damaged nerves. They don’t replace the time that nerve regeneration takes after PTS, and they don’t substitute for a properly structured rehabilitation programme.
What they do is optimise the conditions for recovery. They give the brain the best possible information during the rehabilitation process. Think of it like this: if nerve regeneration is the road being rebuilt, tactile cues are making sure the GPS is updated as the new roads come online. Without that updating process, you can have a perfectly regenerated nerve but still struggle with function because the brain’s maps haven’t caught up [5].
However it’s also worth saying that the research on tactile cues specifically for PTS is still emerging. Most of the evidence comes from broader peripheral nerve injury research and from cortical plasticity studies. The principles are sound and the mechanisms are well understood, but we need more PTS-specific trials. We’re honest about that because we think transparency about the evidence matters more than making bold claims. If you’ve been dealing with chronic pain for a while, you’ll probably appreciate that honesty.
Likewise, tactile cues work best as part of a broader approach. They complement motor learning, graded exposure, pacing strategies, and addressing the psychological components of recovery. The brain’s role in pain and recovery goes well beyond just cortical mapping, and for those dealing with the emotional toll of a PTS diagnosis, the impact of medical trauma needs to be addressed alongside the physical rehabilitation.
Common Questions About Tactile Cues
Do tactile cues actually work or is it just placebo?
The cortical mapping changes are measurable on fMRI, so there is a genuine neurological mechanism at work [2]. That said, there’s almost certainly a confidence component as well, people often feel more secure with a band or tape in place, and that reduction in threat perception probably contributes to the improved movement. But we’d argue that’s not “just” placebo, it’s the nervous system responding to better information. Both mechanisms are real and both are useful.
Can I use tactile cues at home or do I need a practitioner?
Many tactile cue techniques can be used at home. Resistance bands, tape, and textured surfaces are all accessible. However, the tricky part is knowing which cue to use, where to place it, and how to progress over time. Getting the initial setup right with someone who understands the approach makes a big difference. After that, most of the day-to-day work can be done independently.
How long before I notice results?
This is the question everyone asks, and it’s hard to give a straight answer. Some people notice immediate improvements in movement quality during a session. Lasting cortical changes take longer, weeks to months of consistent practice. For those recovering from PTS, the timeline is also influenced by the rate of nerve regeneration, which you can read about in our recovery phases article. When it comes to expectations, think of it as months not days for meaningful structural change.
Are tactile cues the same as proprioceptive training?
They’re related but not identical. Proprioceptive training is the broader category, it includes balance work, joint position sense exercises, and movement control drills. Tactile cues are a specific tool used within proprioceptive training. They enhance the sensory input available to the brain during movement. You could do proprioceptive training without tactile cues, but we’ve found they make it significantly more effective, particularly for those with hypermobility where baseline proprioception is already reduced.
Will tactile cues help with the pain from PTS?
The relationship between cortical mapping and pain is well established. The Lustenhouwer study showed that decreased visuomotor cortical activity correlated directly with increased persistent pain in neuralgic amyotrophy patients [2]. So interventions that improve cortical mapping may also help with pain. However, acute PTS pain is a different beast and needs to be managed with appropriate medical support, particularly as the neuropathic pain can radiate into areas like the upper back and coat hanger region. Tactile cues are more relevant during the rehabilitation and recovery phases than during the initial acute pain period. For those dealing with complex pain conditions like CRPS, there are similar cortical mechanisms at play.
Where to Go From Here
Tactile cues are one piece of a much larger picture. If you’re recovering from Parsonage Turner syndrome, our complete PTS guide is the best place to start. From there, the articles on brain changes and sensory mapping, exercise and rehabilitation, getting the right diagnosis, and the COVID-19 connection will give you the full picture.
For those with hypermobility who aren’t dealing with PTS but want to understand the approach we take, our articles on exercise principles, core stability, and shoulder blade work all use tactile cues as a fundamental part of the approach.
And if you’d like to work with us directly, whether it’s for PTS recovery, hypermobility rehabilitation, or chronic pain management, we’re here to help. The nervous system is at the centre of everything we do and tactile cues are one of the key tools we use to work with it rather than around it.
If nothing else, remember this: your brain can change. The maps can be rebuilt. And giving your nervous system better information is one of the most powerful things you can do for your recovery.
– The Fibro Guy Team –
Where to Go From Here
If you’re working through recovery from Parsonage-Turner syndrome, the principles we use in our studios — neuron-first rehab, sensory mapping, graded loading — are the same ones that underpin our Hypermobility 101 course. It covers the frameworks for rebuilding joint control and proprioception that are directly relevant to PTS recovery. Have a look through the full course library for everything we offer.