Last updated May 2026
Key Takeaways
- POTS is diagnosed when heart rate increases by 30 or more beats per minute within 10 minutes of standing, in the absence of orthostatic hypotension.
- There are three main types of POTS: neuropathic, hyperadrenergic, and hypovolaemic, each with different underlying mechanisms and different treatment implications.
- Up to 50% of people with POTS also have joint hypermobility, likely due to connective tissue laxity affecting blood vessel compliance.
- The Levine Protocol, a structured exercise programme starting with recumbent activity and progressing to upright exercise, has the strongest evidence base for treatment, with 53 to 71% achieving remission in trials.
- POTS, hypermobility/EDS, and mast cell activation syndrome (MCAS) frequently co-occur, sometimes called the “trifecta” or “triad”.
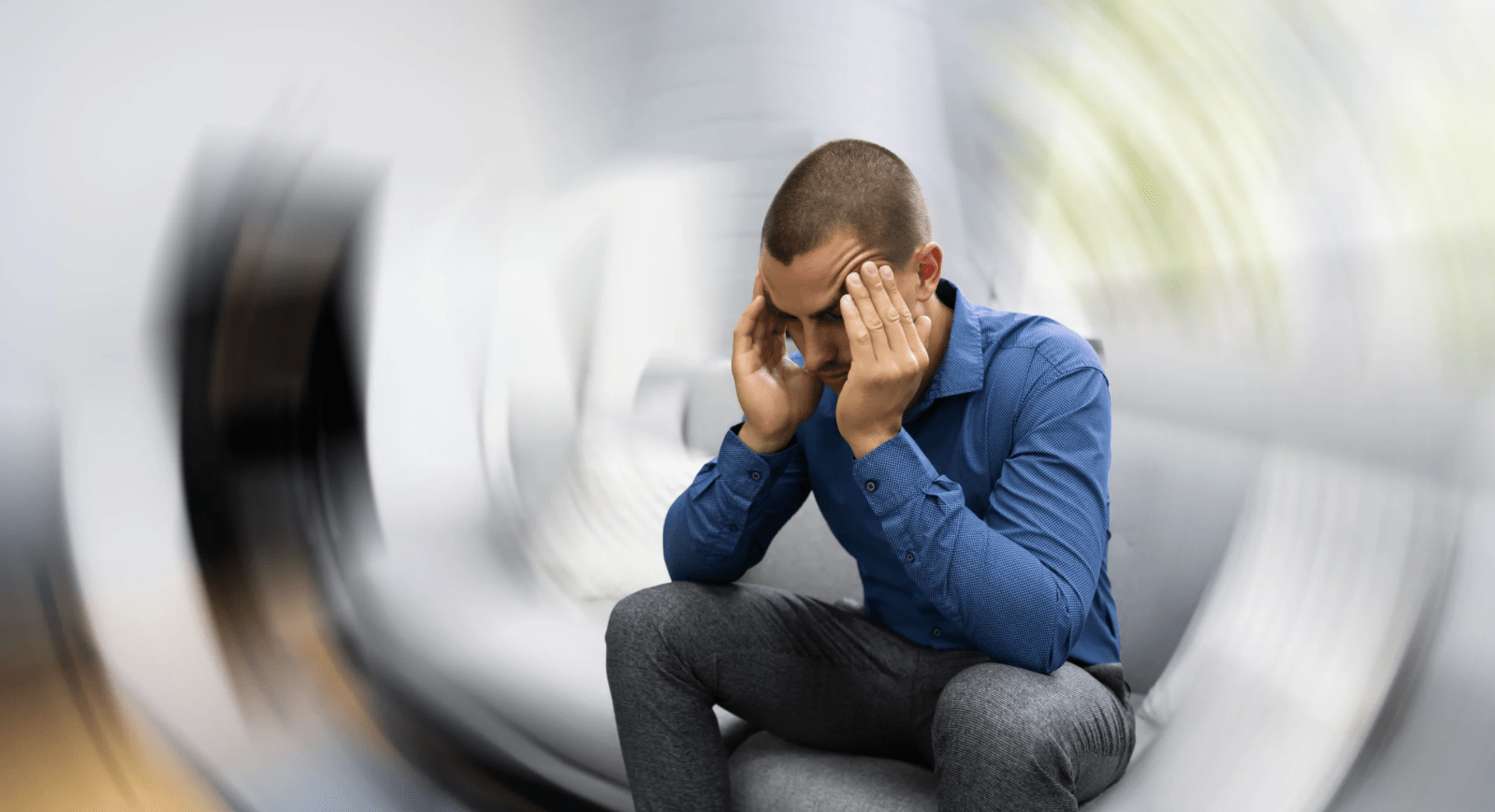
You stand up. In those first few seconds, nothing. Then it starts. Your heart rate climbs, your vision blurs at the edges, a wave of heat or dizziness sweeps through you, and your heart is hammering as though you have just sprinted for a bus. You have not. You have just got up from the sofa.
That experience is one of the most commonly reported, and most misunderstood, symptoms in the hypermobility world. It has a name: Postural Orthostatic Tachycardia Syndrome, or POTS. It is a form of dysautonomia, which is a broad term for when the autonomic nervous system does not regulate the body’s automatic functions properly.
POTS is not rare. It is not “just anxiety.” It is not something you can think your way out of. It is a genuine, physiologically measurable condition that affects an estimated one to three million people in the United States alone [1, 13], and is far more common in those with hypermobility and EDS than in the general population [2].
This is your starting point. We have pulled together everything you need to know about POTS and dysautonomia into one place. Each section expands when you click it, and links to a deeper article if you want to go further. Pick the topics that matter to you and skip what does not.
What Is POTS?

You stand up. In those first few seconds, nothing. Then it starts. Your heart rate climbs, your vision blurs at the edges, a wave of heat or dizziness sweeps through you, and your heart is hammering as though you have just sprinted for a bus. You have not. You have just got up from the sofa. That experience has a name: Postural Orthostatic Tachycardia Syndrome.
Read MorePOTS stands for Postural Orthostatic Tachycardia Syndrome. Broken down: postural means related to body position, orthostatic means upright or standing, and tachycardia means a fast heart rate. The syndrome part reflects the fact that it is a cluster of symptoms with an underlying physiological cause.
Formally, POTS is defined as a heart rate increase of at least 30 beats per minute (bpm) within ten minutes of standing, without a significant drop in blood pressure. In adolescents aged 12 to 19, the threshold is 40 bpm. Symptoms must have been present for at least three months and include frequent lightheadedness, palpitations, brain fog, fatigue, or tremulousness, all of which get worse upright and improve when lying down [1].
That 30 bpm figure is important. A normal heart rate response to standing is an increase of around 10 to 20 bpm. In POTS, the response is excessive, and the heart is essentially trying to compensate for something going wrong in the circulation. When it comes to understanding which subtype you have, that something matters quite a lot.
The Three Main Types of POTS
POTS is not a single condition with one cause. It is better understood as a “final common pathway” that several different mechanisms can produce [12]. The three main subtypes are:
- Neuropathic POTS: Partial sympathetic denervation of the lower limbs. The nerves responsible for constricting blood vessels in the legs and abdomen do not work properly, so blood pools downward when you stand. The heart races to compensate.
- Hyperadrenergic POTS: Driven by excess sympathetic nervous system activity. Norepinephrine levels in the blood are markedly elevated on standing. These patients often have high blood pressure (rather than low), pronounced anxiety-like symptoms, tremor, and headaches.
- Hypovolaemic POTS: The blood volume is genuinely lower than it should be. This makes it even harder to maintain circulation when standing. It is commonly seen alongside low renin and aldosterone levels.
In practice, many people have a mix of these mechanisms, and they can overlap with connective tissue disorders in ways that complicate the picture further [13]. Understanding which subtype predominates actually matters quite a bit, because the same medication that helps one person can make another significantly worse.
→ Read the full guide on exercise for POTS and the first step everyone misses
What Is Dysautonomia?
Dysautonomia is the umbrella term for any dysfunction of the autonomic nervous system. POTS is one of the most common forms, but it is far from the only one. Understanding what dysautonomia actually means puts POTS in its proper context.
Read MoreThe autonomic nervous system (ANS) controls everything your body does automatically: heart rate, blood pressure, breathing rhythm, digestion, temperature regulation, bladder function, and more. It does this through two main branches. The sympathetic nervous system (often called “fight or flight”) accelerates things: it speeds up the heart, raises blood pressure, and redirects blood to the muscles. The parasympathetic system (often called “rest and digest”) does the opposite: it slows things down and promotes recovery and digestion.
In healthy people, these two systems work in a constant, seamless dialogue, adjusting to every change in posture, temperature, stress level, and activity. In people with dysautonomia, that dialogue breaks down. The responses are too big, too small, too slow, or simply wrong for the situation.
Other Forms of Dysautonomia
Other forms of dysautonomia include orthostatic hypotension (blood pressure drops on standing), neurocardiogenic syncope (fainting via vagal response), and multiple system atrophy (a progressive neurological condition). POTS is by far the most commonly encountered in the hypermobility community, though heart rate variability (HRV) changes and other subtle autonomic disturbances are also very common.
Because dysautonomia covers such a wide spectrum of presentations, it is easy to have symptoms that sit within it without receiving a clear label. POTS is the most diagnosable form precisely because it has a measurable criterion: the 30 bpm threshold on standing. Many people with autonomic dysfunction sit just below that threshold, or experience symptoms that are clearly autonomic in origin but do not fit neatly into any single category.
→ Read more on heart rate variability and autonomic function
The POTS-Hypermobility Connection

If you have EDS or HSD, you are significantly more likely to have POTS than someone in the general population. This is not just clinical observation. The data backs it up, and the mechanism is well understood.
Read MoreA 2020 study by Miller and colleagues evaluated 91 adults with POTS using the 2017 hEDS diagnostic checklist. 31% met formal criteria for hEDS, and an additional 24% had generalised joint hypermobility without meeting the full criteria [2]. So roughly half of all POTS patients in that study had some form of hypermobility.
In a large paediatric cohort of 362 young people with POTS, 22.7% had EDS and 39% had HSD, meaning over 60% had some form of hypermobility disorder [3]. Those with EDS also had earlier symptom onset and longer symptom duration. A separate study found that POTS prevalence was significantly higher in young women across the hypermobility spectrum than in healthy controls [19].
And in a 2025 study of women with HSD and hEDS, 58.3% had physician-diagnosed POTS, and one in four had the full clinical triad of hypermobility, POTS, and MCAS [4].
Why Does This Connection Exist?
The leading explanation involves connective tissue. In EDS and HSD, the connective tissue throughout the body is more elastic and less structurally stable than it should be. Blood vessels are also made of connective tissue. When those vessels are more compliant and less supportive, blood tends to pool more readily in the legs and abdomen when you stand up. The veins stretch and widen instead of maintaining tone, and the heart has to work harder to maintain circulation to the brain.
This is sometimes described as “venous pooling”. The upright circulatory system essentially leaks volume downward, triggering the compensatory tachycardia that defines POTS [2, 9].
There is also emerging evidence around small fibre neuropathy (damage to the small autonomic nerve fibres in the skin and tissues), which is more common in hEDS than previously recognised, and may directly impair the blood vessel constriction that is supposed to prevent pooling [1, 13].
It is also worth noting that POTS is increasingly recognised after viral illness. One study found that 79% of long COVID participants met formal POTS criteria, suggesting post-viral illness can unmask autonomic vulnerability in those already predisposed [14]. If you are still piecing together whether your symptoms point towards hypermobility, it is worth reading about the full symptom picture of EDS and HSD and how the diagnosis process works.
How POTS Is Diagnosed

POTS is diagnosed primarily through a sustained orthostatic challenge, measuring what happens to your heart rate when you go from lying down to standing. There are three main methods, each with a slightly different application.
Read MoreThe Active Stand Test
This is the simplest and most commonly used. You lie flat for at least five to ten minutes while your heart rate and blood pressure are measured. You then stand and measurements are taken at one, three, five, eight, and ten minutes. A sustained rise of at least 30 bpm (or 40 bpm in teenagers) on at least two of those readings, without a significant blood pressure drop, confirms POTS [1].
The Tilt Table Test
A more controlled version. You are strapped to a table that tilts you to 60 to 70 degrees upright. This removes the effect of muscle pumping from the legs (which would normally help return blood to the heart during active standing), making it a purer test of autonomic cardiovascular control. It is used when the active stand result is equivocal or when additional detail is needed.
The NASA Lean Test
A simplified version of the tilt table that can be done at home or in a GP surgery. You lean against a wall at roughly 70 to 75 degrees while heart rate is measured over ten minutes. It is not quite as standardised as the active stand or tilt table, but it is useful when formal testing is not immediately available.
Before the test, it is standard to rule out other causes of tachycardia: anaemia, thyroid dysfunction, dehydration, medications, and arrhythmias all need to be excluded. POTS is a diagnosis of the pattern of response, not just an isolated fast heart rate [1].
It is worth noting that because many people with EDS are diagnosed via specialist referral, there can be a significant delay between symptom onset and formal diagnosis. If you are seeking a pathway to diagnosis, understanding how EDS and HSD are formally assessed can help you have more productive conversations with your doctors.
Common Symptoms of POTS

The hallmark symptom is a pounding, racing heart when you stand up or have been upright for a while. But POTS produces a much broader symptom picture than just tachycardia, and for many people it is the non-cardiac symptoms that are most disabling.
Read MoreThe core symptom cluster includes tachycardia and palpitations on standing, but POTS produces a much broader picture. Symptoms tend to be worse first thing in the morning, in hot conditions, after eating large meals, and during periods of physical deconditioning. They are generally better when lying down, during cool weather, and when physically conditioned.
- Tachycardia and palpitations: The heart rate spikes on standing and may stay elevated throughout the time you are upright. Some people describe their heart “fluttering” or pounding against their chest.
- Lightheadedness and pre-syncope: That dizzy, faint-feeling sensation when you stand, sometimes to the point of blacking out. It is caused by reduced blood flow to the brain.
- Brain fog: Difficulty concentrating, slow thinking, memory problems. This is covered in its own section below.
- Fatigue: Severe, disproportionate exhaustion that does not fully resolve with rest. Dysautonomia is physically demanding: the body is constantly working hard just to maintain basic circulation.
- Coat hanger pain: Aching pain across the neck, shoulders, and upper back, often described as resembling the shape of a coat hanger. It is caused by reduced blood flow to the muscles of the upper trapezius area when the body prioritises circulation elsewhere.
- Heat intolerance: Heat causes blood vessels to dilate further, worsening the pooling problem. Many people with POTS feel much worse in summer, hot showers, or warm environments. There is quite a lot written on why heat intolerance is so common across these conditions.
- Cold intolerance: Less intuitive but also common. Cold intolerance is often driven by poor peripheral circulation and dysregulated temperature control.
- Blood pooling: The legs and feet can turn a mottled red-blue (livedo reticularis) when standing, as blood pools in the small vessels. Some people find their feet visibly change colour within minutes of standing.
- Nausea and GI symptoms: The autonomic nervous system controls gut motility. Dysautonomia disrupts this, leading to nausea, bloating, gastroparesis, and constipation. If you have also been offered a GLP-1 receptor agonist like Ozempic or Wegovy, the gut-slowing effect of those drugs is something we cover in depth here, because it sits on top of whatever is already going on with POTS-related motility. For the constipation side of the autonomic picture specifically, see our guide to constipation in hypermobility, EDS and POTS.
- Shortness of breath: Even at rest, but particularly on standing or mild exertion. Often linked to the breathing pattern changes covered later in this guide.
- Anxiety-like symptoms: Hyperadrenergic POTS in particular can produce surges of adrenaline that feel indistinguishable from a panic attack. The relationship between hypermobility and anxiety runs deep and is worth understanding properly.
→ Read the full guide on coat hanger pain and why it happens
Brain Fog: The Cognitive Cost
Brain fog is one of the most debilitating features of POTS, and for a long time it was dismissed or attributed to anxiety. The research now tells a clearer story: there is a measurable physiological cause rooted in blood flow.
Read MoreWhen you stand up, blood needs to be actively redirected to the brain against gravity. In POTS, this process is impaired. Cerebral blood flow drops, and the brain does not get the oxygen and glucose it needs to function properly. You feel slow, foggy, and unable to concentrate, not because something is psychologically wrong, but because your brain is quite literally getting less blood than it needs [6].
What the Research Shows
A 2020 study by Wells and colleagues demonstrated this directly. POTS patients showed a 7.8% reduction in cerebral blood flow velocity after a prolonged cognitive stress test, compared to just 1.8% in healthy controls. This translated into measurable psychomotor slowing and increased difficulty concentrating, and crucially, these effects occurred even while seated, not just on standing [6].
A 2025 SPECT imaging study went further, finding that 61% of POTS patients had abnormal cerebral blood flow even while lying down, not just on standing. The most affected regions were the lateral prefrontal cortex (associated with attention, working memory, and executive function) and the sensorimotor cortex [7]. This helps explain why brain fog in POTS is not just an “upright” problem. For many people, it is present to some degree all the time.
There is also a CO2 connection here, which is covered in the next section. When it comes to practical strategies for managing brain fog day to day, the detailed guide on brain fog in EDS, POTS, and long COVID covers the mechanisms and practical approaches in much more depth.
→ Read the detailed guide on brain fog in EDS, POTS, and long COVID
Why Is Blood Pressure Often Low?

POTS is technically defined as tachycardia without a significant blood pressure drop. But many people with POTS do have low blood pressure, particularly when upright, and it is worth understanding why the two so often travel together.
Read MoreIn hyperadrenergic POTS, blood pressure can actually be elevated. But in neuropathic and hypovolaemic subtypes, the inability of blood vessels to constrict properly on standing means that while the heart rate goes up (the compensatory mechanism), the blood pressure stays lower than it ideally should be. The tachycardia is essentially the body’s attempt to maintain adequate output despite low filling pressure.
Chronically low blood pressure, particularly when combined with poor circulation, contributes to fatigue, cognitive impairment, and that pervasive sense of not having enough energy for anything. For a deeper dive into the mechanisms behind low blood pressure and its wider effects on chronic pain and fatigue, that is covered separately.
Supine Hypertension
It is also worth noting that some people have what is called supine hypertension: normal or elevated blood pressure when lying down, dropping to lower levels on standing. This is particularly common in hyperadrenergic POTS and creates a management challenge, because treatments that raise blood pressure (like fludrocortisone) can make this worse. It is one of several reasons why POTS management really does need to be subtype-specific, and why blanket advice does not always serve people well.
→ Read the full guide on low blood pressure and its effects on chronic pain and fatigue
Salt and Fluid: What the Science Actually Says

You have almost certainly been told to increase salt and water intake for POTS. This recommendation appears in virtually every POTS management guide, and it is not wrong, but the picture is more complicated than the advice usually suggests.
Read MoreThe rationale is straightforward: more sodium in the bloodstream helps retain water through the kidneys, which expands plasma volume. Expanded plasma volume means more blood available to circulate when you stand. The heart does not need to race as hard.
What the Research Actually Found
A well-designed 2021 crossover trial by Garland and colleagues tested this directly. When POTS patients followed a high-sodium diet (300 mEq/day) compared to a low-sodium diet (10 mEq/day), their heart rate increase on standing dropped from 60 to 46 bpm, plasma volume improved, and standing norepinephrine decreased. These are meaningful improvements [8].
However, and this is worth emphasising: even on the high-sodium diet, POTS patients’ upright heart rates (117 bpm) and orthostatic tachycardia (46 bpm) remained significantly higher than healthy controls (85 bpm, 19 bpm increase). Salt helps, but it does not fix POTS on its own. It is a supportive measure, not a cure [8].
Current guidelines recommend 3 litres of fluid per day and 5 to 10 g of salt per day for most adults with POTS [1]. Electrolyte drinks can help with compliance. For people with the hypovolaemic subtype, this is particularly important. For much more detail on the research, including which forms of salt are most useful and how to approach this practically, the full guide on salt in POTS is worth reading.
Exercise: The Most Evidence-Based Treatment
Exercise is, without question, the most evidence-based intervention for POTS. It is also the one most likely to provoke disbelief in people who have tried to exercise and felt dramatically worse. Understanding why requires understanding the deconditioning cycle.
Read MoreThe reason so many people with POTS feel awful when they exercise is that they try to walk, stand, or do upright cardio, which immediately triggers their symptoms. The research is clear that the starting point matters enormously.
The Deconditioning Cycle
POTS is both caused and worsened by physical deconditioning. When you feel awful standing up, you naturally spend more time lying down. But lying down causes the heart to shrink slightly (cardiac atrophy), blood volume to decrease, and the muscles that pump blood back from the legs to weaken. All of which makes POTS worse, which makes you spend more time lying down, which makes everything worse again.
Research by Levine and colleagues at UT Southwestern demonstrated this clearly. POTS patients had significantly smaller hearts and lower blood volumes than healthy sedentary controls matched for age and sex. When those patients underwent a structured three-month exercise programme, their cardiac size and mass increased by around 12% and 8% respectively, their blood volume increased by 6%, and their peak VO2 improved by 8% [20]. Most importantly, 53 to 71% achieved remission of POTS by the end of the three months [9].
A 2025 systematic review confirmed that exercise is now considered first-line non-pharmacological treatment for POTS [10], and a 2023 randomised controlled trial found that a personalised, semi-supervised exercise programme produced significantly better improvements in aerobic fitness, orthostatic symptoms, and exercise tolerance than standard care [11].
The Levine Protocol: How It Works
The key to the protocol is starting horizontal. The Levine approach bypasses the symptom-triggering problem by beginning with exercise that does not require you to be upright [9].
In the first month or two, everything is horizontal or recumbent: rowing machines, recumbent bikes, swimming. This allows the cardiovascular system to begin adapting without the orthostatic challenge that causes symptoms. As fitness improves and heart size and blood volume increase, upright exercise is gradually introduced.
- Month 1: 3 to 4 sessions per week, 20 to 30 minutes of recumbent cardio, plus basic lower body and core resistance work. All seated or lying.
- Month 2: Increase duration and add a second resistance session. Begin adding upright exercise if tolerated.
- Month 3: 5 to 6 sessions per week, 35 to 60 minutes per session. Mix of recumbent and upright cardio. Maintain resistance training.
The resistance work is specifically for the lower body and core, because the leg muscles act as a venous pump. Stronger legs means better blood return to the heart on standing, which reduces the tachycardia [9].
For those with EDS or HSD, non-weight bearing options like swimming and rowing are particularly useful given the joint considerations involved. The full guide on exercise for POTS covers how to adapt this for hypermobility, including the specific first steps most people miss.
If you are new to exercise in this context, the broader starting exercise with hypermobility guide is a sensible starting point.
→ Read the full guide on exercise for POTS, including the first step most people miss
CO2 Tolerance and Breathing
There is a breathing component to POTS that does not get nearly enough attention, and the research on it is genuinely striking. Many people with POTS breathe in patterns that actively worsen their symptoms.
Read MoreMany people with POTS breathe in a pattern that keeps their CO2 levels lower than optimal. This might not sound like a big deal, CO2 is just what you breathe out, right? But CO2 is one of the primary signals the blood vessels use to regulate their diameter. Low CO2 causes blood vessels to constrict, including the cerebral vessels. It also increases heart rate.
The Research
A 2023 clinical study demonstrated this directly in POTS patients: when CO2 was experimentally lowered (hypocapnia), heart rate rose from 82 to 99 bpm, and stroke volume fell, possibly because of increased blood pooling in the capacitance vessels [16]. Another systematic review found consistent evidence linking hypocapnia to tachycardia specifically in POTS [15].
This means that dysfunctional breathing patterns, overbreathing in particular, can actively worsen POTS symptoms. It is not just a co-occurring problem. When it comes to managing POTS, breathing retraining to improve CO2 tolerance can make a meaningful difference to both symptoms and exercise capacity. The full guide on CO2 tolerance and its impact on breathlessness, fatigue, and chronic pain is worth reading alongside this page.
→ Read the full guide on CO2 tolerance, breathlessness, fatigue, and chronic pain
MCAS: The Third Part of the Triangle

In many clinical and patient communities, you will hear about a triad: hEDS/HSD, POTS, and Mast Cell Activation Syndrome. The clinical overlap between these three conditions is real and well-documented.
Read MoreMast Cell Activation Syndrome is a condition in which mast cells (immune cells involved in allergic responses) trigger excessively or without a clear cause, releasing histamine and other inflammatory mediators in ways that produce wide-ranging symptoms.
How Common Is the Overlap?
The clinical overlap between hEDS/HSD, POTS, and MCAS is real and well-documented. A 2025 study of 84 women with HSD or hEDS found that 25% had all three diagnoses: hypermobility, POTS, and MCAS [4]. In a large paediatric POTS cohort, the frequency of MCAS varied from 2% to 87% depending on which diagnostic criteria were used, highlighting both the genuine overlap and the diagnostic uncertainty [5]. For a fuller breakdown of how these three conditions interact, see POTS, EDS and MCAS: understanding the trifecta.
A 2021 study of 69 adult POTS patients found that 64% had non-orthostatic symptoms consistent with mast cell activation (including migraines, allergic complaints, skin rashes, and gastrointestinal symptoms), and 42% had both symptoms and at least one elevated biochemical marker (elevated prostaglandins, histamine, or methylhistamine) [17].
Why Do These Three Conditions Cluster Together?
One hypothesis involves the connective tissue: mast cells are concentrated in connective tissue, and in EDS/HSD, there may be local tissue changes that encourage mast cell dysregulation. There is also likely a bidirectional relationship; mast cell mediators can directly affect blood vessel tone and autonomic function, potentially worsening POTS [17].
It is worth being clear that the research on this triad is still evolving. Diagnostic criteria for MCAS remain contested, and not every claim you will see online about this overlap is based on solid evidence. The full guide on MCAS walks through what is actually established and what is still speculative.
→ Read the full guide on MCAS, what is established and what is still speculative
Medication Overview
Several medications are used to manage POTS symptoms. None cure POTS, and most are used off-label. They are generally employed to reduce symptom burden while lifestyle and exercise approaches take effect.
Read MoreThis section is for information only and is not medical advice. Medication decisions should always be made with a qualified clinician who knows your specific situation.
Several medications are used to manage POTS symptoms. None of them cure POTS, and none are approved by most regulatory bodies specifically for POTS (meaning they are used off-label). They are generally used to reduce symptom burden while lifestyle and exercise approaches take effect.
Beta Blockers (e.g. Propranolol)
The most commonly prescribed first-line medications. Beta blockers reduce the heart rate response to standing by blocking the effects of adrenaline on the heart. Low-dose propranolol (10 to 20 mg, up to four times daily) has moderate evidence behind it and is the Canadian Cardiovascular Society’s recommended first-line medication option [1]. It is particularly useful for hyperadrenergic POTS. It should be avoided in people with asthma or very low heart rate at baseline.
Ivabradine
A more selective heart rate reducer that does not block adrenaline receptors, making it useful for people who do not tolerate beta blockers. It targets the “funny current” in the heart’s pacemaker cells specifically. Evidence quality is moderate [1], and it is generally better tolerated than propranolol for people with hypermobility-related exercise intolerance. For a full breakdown of the trials, the dosing, and where the evidence is genuinely strong, see our guide to what the evidence actually says about ivabradine for POTS.
Fludrocortisone
A synthetic mineralocorticoid that promotes sodium and water retention by the kidneys, effectively expanding blood volume. It addresses the hypovolaemia component of POTS. Electrolyte monitoring (particularly potassium) is important. It can worsen supine hypertension and is not appropriate for hyperadrenergic POTS [1].
Midodrine
A vasoconstrictor that works by constricting the blood vessels in the periphery, reducing the pooling problem. It is taken during the day (not near bedtime, because it raises blood pressure and can cause supine hypertension). Particularly useful for neuropathic and hypovolaemic subtypes [1].
Other options include pyridostigmine (improves nerve-to-blood vessel communication), clonidine or methyldopa (for hyperadrenergic POTS), and in some cases, low-dose desmopressin for severe hypovolaemia. Most people will try lifestyle measures first, then add medication if needed. The 2026 POTS guidelines brought some useful updates to how medication is sequenced. The full breakdown of what changed in the 2026 guidelines is worth reading for anyone currently navigating treatment options.
→ Read the 2026 POTS guidelines: what changed and what it means for treatment
Living With POTS Daily
Beyond exercise, salt, and medication, there are several practical strategies that make a real difference to day-to-day life with POTS. The physical side is only part of the picture.
Read MorePacing
One of the most important concepts for anyone with POTS. Pacing means deliberately managing your activity levels to avoid triggering post-exertional crashes. This is not about resting more; it is about distributing activity more intelligently. The complete guide to pacing for EDS and chronic pain covers the evidence and practical strategies. For POTS, horizontal rest breaks throughout the day (not just at the end) can significantly reduce symptom burden.
Compression Garments
Waist-high compression garments (not just below-the-knee stockings) reduce blood pooling by applying external pressure to the legs and abdomen. Research suggests abdominal compression is particularly important, as a significant proportion of blood pools in the abdominal veins, not just the legs [1, 9]. Medical-grade garments (20 to 30 mmHg or higher) are more effective than standard compression stockings from a chemist. For a deeper look at what the evidence does and does not support for compression in POTS, hypermobility and EDS, see compression garments for hypermobility, EDS and POTS.
Sleep Positioning
Sleeping with the head of the bed raised by 10 to 20 degrees (physically raising the head end, not just using pillows) encourages the kidneys to retain more sodium overnight, which helps maintain plasma volume during the day. This is called “nocturnal anti-Trendelenburg positioning” in the literature. It is a small change that can have a meaningful cumulative effect. Sleep itself is often disrupted in POTS, and we have covered this in detail in POTS and sleep: why rest does not come easily, alongside the broader picture of sleep in hypermobility.
Diet Timing and Composition
Large meals divert significant blood flow to the gut for digestion, worsening circulatory distribution. Eating smaller, more frequent meals reduces this effect. High-carbohydrate meals are particularly problematic. Salt-loading before anticipated upright activity (such as before exercise or a long day out) can preemptively boost plasma volume. For more on dietary approaches in hypermobility-related conditions, the hypermobility and diet guide covers this well.
Managing Flares
POTS symptoms tend to flare with infections, heat, dehydration, sleep deprivation, and significant stress. Having a flare plan helps: oral rehydration salts, horizontal rest, compression, reduced activity, and not abandoning the exercise programme entirely but scaling back temporarily. The guide on managing EDS flares is applicable here. Avoid the trap of complete rest for extended periods; this accelerates deconditioning and makes recovery harder.
Physical Countermeasures
Simple physical manoeuvres can acutely reduce symptoms: leg crossing, calf raises, squatting, or tensing the leg muscles all increase venous return and can buy you time in situations where you need to stand. Some people find cooling strategies (cool packs, cold water on the face or neck) helpful for managing heat-triggered symptoms.
Napping is a double-edged sword. Short naps can help manage fatigue, but excessive horizontal time feeds deconditioning. There is some practical guidance on this in the guide on napping in chronic conditions.
When it comes to the broader musculoskeletal picture, understanding the mechanisms behind chronic pain in fibromyalgia and hypermobility is valuable context for anyone navigating multiple overlapping diagnoses. And for those interested in nutritional support alongside exercise, creatine for hypermobility and EDS has some genuinely useful research behind it.
→ Read the complete evidence-based pacing guide for EDS and chronic pain
Chronic Pain, Relationships and Intimacy

The bit of chronic pain that gets skipped in clinic is the bit that affects your relationship, your sex life, and how you talk about any of it with the person you share a bed with. Sleep gets asked about. Walking the dog gets asked about. The fact your hip subluxes when you change position, or that you crash for three days after anything more than a cuddle, somehow does not.
That gap is where most of the hidden suffering sits, and it shows up across hypermobility, fibromyalgia, POTS and ME/CFS. We have a full guide covering disclosure to new partners, communication inside long term relationships, positioning, pacing intimacy, the LGBTQ and polyamorous experience of chronic pain, and how to look after a body that does not always cooperate. The pacing piece is particularly relevant to POTS and ME/CFS: see pacing intimacy with POTS, fatigue, and ME/CFS for the practical detail.
→ Read the full guide: Chronic Pain, Relationships and Intimacy
Where to Go From Here
POTS is one of those things where actually understanding what is going on makes a significant difference to how you manage it. And if you have hypermobility alongside it, which statistically most of you reading this will, the exercise approach needs to account for both.
The Hypermobility Live Workshop covers POTS as part of the bigger picture. Four weeks, live sessions, and you can ask us about your specific symptoms. It is what we do in our studios, just online. Or have a browse through the course library for self-paced options.
Free exercises and practical tools are on the Hypermobility Resources page.

Ready to work through this with structure and support?
The Hypermobility Live Workshop is four weeks of breaking down the frameworks we use in our studios, with live Q&A so you can ask about your specific situation. Two free courses are included.
References
- Raj SR, Fedorowski A, Sheldon RS (2022) ‘Diagnosis and management of postural orthostatic tachycardia syndrome’, CMAJ, 194(10), pp. E378-E385. doi: 10.1503/cmaj.211373
- Miller AJ, Stiles LE, Sheehan T, Bascom R, Levy HP, Francomano C, Arnold AC (2020) ‘Prevalence of hypermobile Ehlers-Danlos syndrome in postural orthostatic tachycardia syndrome’, Auton Neurosci, 224, p. 102637. doi: 10.1016/j.autneu.2020.102637
- Boris JR, Bernadzikowski T (2021) ‘Prevalence of joint hypermobility syndromes in pediatric postural orthostatic tachycardia syndrome’, Auton Neurosci, 231, p. 102770. doi: 10.1016/j.autneu.2020.102770
- Collins Hutchinson ML, Liang E, Fuster E, Blitshteyn S (2025) ‘Autonomic symptom burden, comorbidities and quality of life in women with Hypermobility Spectrum Disorders and hypermobile Ehlers-Danlos syndrome’, Auton Neurosci, 262, p. 103356. doi: 10.1016/j.autneu.2025.103356
- Yao L, Subramaniam K, Raja KM, et al. (2025) ‘Association of postural orthostatic tachycardia syndrome, hypermobility spectrum disorders, and mast cell activation syndrome in young patients’, Front Neurol, 16, p. 1513199. doi: 10.3389/fneur.2025.1513199
- Wells R, Malik V, Brooks A, et al. (2020) ‘Cerebral Blood Flow and Cognitive Performance in Postural Tachycardia Syndrome: Insights from Sustained Cognitive Stress Test’, J Am Heart Assoc, 9(13), p. e017861. doi: 10.1161/JAHA.120.017861
- Seeley MC, O’Brien H, Wilson G, et al. (2025) ‘Novel brain SPECT imaging unravels abnormal cerebral perfusion in patients with postural orthostatic tachycardia syndrome and cognitive dysfunction’, Sci Rep, 15, p. 3487. doi: 10.1038/s41598-025-87748-4
- Garland EM, Gamboa A, Nwazue VC, et al. (2021) ‘Effect of High Dietary Sodium Intake in Patients With Postural Tachycardia Syndrome’, J Am Coll Cardiol, 77(20), pp. 2540-2551. doi: 10.1016/j.jacc.2021.03.005
- Fu Q, Levine BD (2018) ‘Exercise and non-pharmacological treatment of POTS’, Auton Neurosci, 215, pp. 20-27. doi: 10.1016/j.autneu.2018.07.001
- Cortez MM, Arnold AC, Boris JR, Davenport TE, et al. (2025) ‘Impact of exercise to treat postural orthostatic tachycardia syndrome: a systematic review’, Front Neurol, 16, p. 1567708. doi: 10.3389/fneur.2025.1567708
- Wheatley-Guy CM, Shea MG, Parks JK, Scales R, Goodman BP, Butterfield RJ, Johnson BD (2023) ‘Semi-supervised exercise training program more effective for individuals with POTS in randomized controlled trial’, Clin Auton Res, 33(6), pp. 659-672. doi: 10.1007/s10286-023-00970-w
- Narasimhan B, Aggarwal D, Satish P, Kantharia B, Aronow W (2022) ‘Postural orthostatic tachycardia syndrome: pathophysiology, management, and experimental therapies’, Expert Opin Investig Drugs, 31(10), pp. 1017-1025. doi: 10.1080/13543784.2022.2121697
- Sebastian SA, Co EL, Panthangi V, et al. (2022) ‘Postural Orthostatic Tachycardia Syndrome (POTS): An Update for Clinical Practice’, Curr Probl Cardiol, 47(12), p. 101384. doi: 10.1016/j.cpcardiol.2022.101384
- Seeley MC, Gallagher C, Ong E, et al. (2025) ‘High incidence of autonomic dysfunction and POTS in patients with long-COVID’, Am J Med, 136(10), pp. 1059-1067. doi: 10.1016/j.amjmed.2023.06.010
- Ranada S, Lei L, Baker J, et al. (2023) ‘Is there a relationship between hypocapnia and tachycardia in POTS? A systematic review’, Clin Auton Res, 33(2), pp. 191-195. doi: 10.1007/s10286-023-00928-y
- Ranada S, Karalasingham K, Baker J, et al. (2023) ‘Hypocapnia increases heart rate in patients with POTS’, Physiology, 38(S1), p. 5730244. doi: 10.1152/physiol.2023.38.S1.5730244 [Conference abstract]
- Kohno R, Cannom DS, Olshansky B, et al. (2021) ‘Mast Cell Activation Disorder and Postural Orthostatic Tachycardia Syndrome: A Clinical Association’, J Am Heart Assoc, 10(17), p. e021002. doi: 10.1161/JAHA.121.021002
- Meskill G, Rege R, Meskill S (2023) ‘Prevalence of comorbid POTS in narcolepsy’ [Conference abstract], Sleep, 46(Suppl 1), p. A257. doi: 10.1093/sleep/zsad077.0586
- Peebles KC, Tan I, Butlin M, Collins F, Tofts L, Avolio AP, Pacey V (2022) ‘The prevalence and impact of orthostatic intolerance in young women across the hypermobility spectrum’, Am J Med Genet A, 188(6), pp. 1761-1776. doi: 10.1002/ajmg.a.62705
- Fu Q, Levine BD (2015) ‘Exercise in the postural orthostatic tachycardia syndrome’, Auton Neurosci, 188, pp. 86-89. doi: 10.1016/j.autneu.2014.11.008