If you have hypermobility and spend any time online, you’ve almost certainly run into the Body Braid. It’s that spiral elastic garment, the one that wraps round the torso and the limbs, in a sort of figure of eight, and it gets marketed pretty hard to people with hypermobility and EDS. The pitch is a lovely one though; better posture, better balance, and body that finally feels held together rather than held on with sticky tape. And now, apparently, there’s a 2025 study to back the whole thing up.
So, a lot of you have been asking me what I make of it. Is it worth the money? And does the science actually hold up the way the marketing says it does?
This article is my honest answer, and I’m going to go deep, because that’s the only real way to do this properly. I’ve read the study everyone keeps pointing me towards, I’ve read the papers that study leans on (all of them), in full, and I’ve gone through the wider research on balance, gait, and proprioception in this group, so I’m not just giving you an opinion off the top of my head. I’ll name the product, I’ll name the poster, and I’ll tell you exactly where the evidence is strong. I’ll also tell you where it’s wafer thin, and where the marketing claims muchmore than the data can actually back up.
Now,I’ll say this up front, because it matters: I actually rather liked the thing itself. This isn’t me kicking a product I hated, as it’s a well made garment, and that’s exactly why the evidence side is worth getting right.
I’m also going to do something the marketing doesn’t do, which is tell you about three things I genuinely noticed when I put the thing on and wore it out and about. Things that (funnily enough) have far better science behind them than the claims printed on body braid packaging (go figure).
Quick warning before we get stuck in though. This is not medical advice, and it’s not me telling you whether you, specifically, should buy one. People are different, bodies are different, and a garment that does precisely nothing measurable in a lab can still feel genuinely useful to wear about the place. What this is, is a straight, no nonsense look at the evidence (something I am fairly good at and genuinely enjoy), so that you can make your own call with your eyes wide open. When it comes to spending money on hypermobility, that bit matters, because let’s be honest, most of you reading this have already spent an absolute fortune on things that promised the earth and delivered very little.
First, the thing itself
Before we get anywhere near the science, let me tell you what it’s actually like in the hand and on the body, because this part genuinely surprised me. I was impressed with the material and the quality of it. It’s far more comfortable than you would think, which is not a given with this sort of garment, and both Jonny and I wore the same medium and got it to fit using the adjustment straps. It’s a well designed bit of kit, and that came through the moment we put it on.
There’s a nice touch on the Corebraid version as well: you can bring the cross straps down lower, so if you’re a bit sensitive across the stomach, you can sit them lower, so that they support your lower back and your hips a little more instead. That sort of adjustability is the kind of thoughtful design detail I like to see.
It’s not perfect by any means though, and I’ll be honest about that as well. The Velcro attachments felt a touch thin to me, and I wasn’t mad keen on the knee and elbow coverage being paid add ons: since the Core braid on its own doesn’t cover them. Small things I know, but worth flagging. So, as a piece of kit I rated it. The questions I’m about to dig into though, are about the claims printed on the website and packaging, not the craftsmanship, and those are two very different things.
What the Body Braid claims
The Body Braid marketing, across the website and the partner pages, rests on three load bearing claims.
The first is that it amplifies proprioception. Proprioception is your brain’s sense of where your body is in space, the thing that lets you touch your nose with your eyes closed, and it’s well documented as being impaired in this group [15]. The braid is said to boost it by giving continuous skin level cues along your fascial lines.
The second claim is mechanical. The braid is said to provide support and “return the spring” to your gait and posture by loading connective tissue along Thomas Myers’ Anatomy Trains model, the idea that there are continuous myofascial chains running through the body.
The third claim is the one that actually matters, because it’s the only one that’s dressed up as evidence based. There’s now a 2025 study, the marketing says, showing the braid improves balance and reduces pain in people with hypermobility.
That third claim is where this appraisal lives. Anyone can make a mechanism sound clever. The question is whether the study they point to does the work they’re asking it to do.
The study everyone points to
So, let’s look at it.
The 2025 evidence is a conference poster by Miller and colleagues, from the Lebanon Valley College Department of Physical Therapy [1]. I want to be precise here, because the word “study” is doing a lot of lifting in the marketing. This is a poster, presented at a college research symposium. It is not a peer reviewed paper. And Body Braid donated the garments used in it, which is disclosed in the acknowledgements, to their credit.
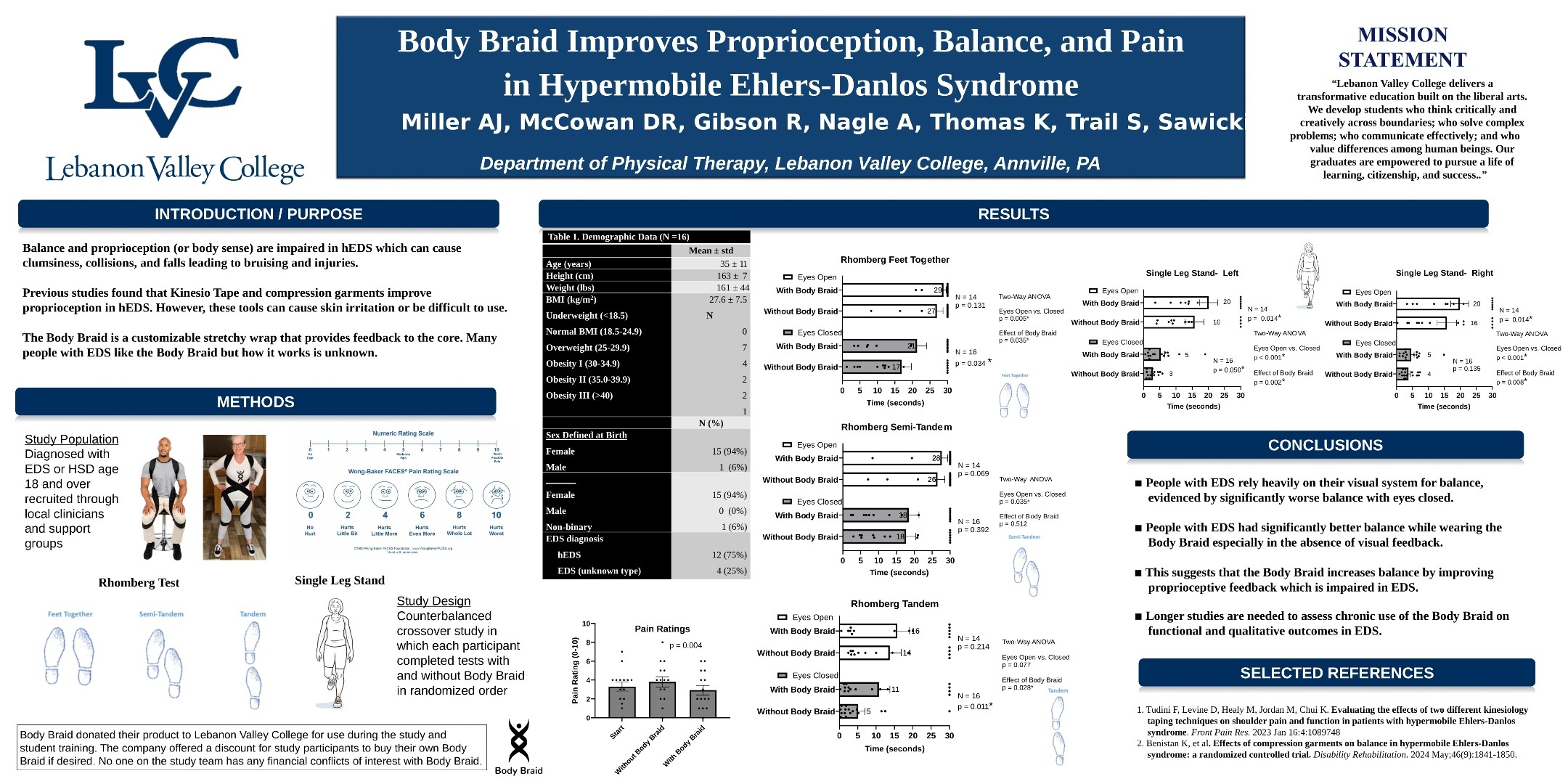
Here’s the design, in brief. Sixteen participants with hypermobility, fifteen female, one non-binary, mean age thirty five. A counterbalanced crossover, so each person was tested both with and without the braid, with the order randomised. The outcomes were a battery of Romberg balance tests, feet together, semi tandem and tandem, with eyes open and eyes closed, plus single leg stance on the left and right, and self reported pain on a Wong-Baker face scale.
The results they report as significant: Romberg feet together with eyes closed (p=0.034), Romberg tandem with eyes closed (p=0.011), single leg stance bilaterally with eyes closed (p<0.001), and pain (p=0.004).
And that, more or less, is the entire academic case for the Body Braid. One poster. Sixteen people. One session.
Why that poster can’t carry the weight
Now, I want to be fair to the people who ran this. A small pilot is a perfectly reasonable thing to do. Sixteen people is fine as a first signal. The problem isn’t that the study exists. The problem is that it’s being used as the evidence base for a commercial product sold to a global hypermobility audience, and it simply isn’t built for that. Here’s why.
The sample is tiny, with no power calculation reported. Sixteen people tells you whether something is worth investigating further. It does not tell you whether a product works, and it certainly doesn’t tell you whether it works for the much wider and more varied population the braid is sold to. A pilot of this size is a starting gun, not a finish line, and it should be read that way rather than waved around as settled science.
It’s a poster, not a paper. This is a bigger deal than it sounds. A conference poster gets a brief look from a symposium committee. It does not get the line by line interrogation that a reviewer at Frontiers or JOSPT or BMC Musculoskeletal Disorders would give it. The statistics, the blinding, the washout, the outcome definitions, none of that gets pulled apart the way it would in a real journal. As far as the academic record shows, this poster has not appeared in any indexed publication as of June 2026. That’s a material gap, not a technicality.
There’s manufacturer involvement, in that the company donated the product. They disclosed it, which is the right thing to do. But a device donation from the manufacturer to a small student led study is exactly the kind of arrangement that introduces allegiance bias, and a peer reviewer would flag it in a heartbeat. A poster doesn’t get that scrutiny.
Everything was measured within a single session. With the braid on, without the braid on, same day, done. There’s no follow up. So, the poster cannot answer the one question that actually matters to those with hypermobility, which is whether wearing the braid produces any lasting change, off the braid, after a period of use. It doesn’t ask, so it can’t tell you.
And here’s the big one. Proprioception was never actually measured, even though the marketing says the braid improves it. The poster measured static balance and a pain face scale. Balance is a downstream behavioural correlate of proprioception, it is not a proprioceptive measure. In the research literature, proprioception is measured with joint position matching, threshold to detection of passive motion, or force matching tasks. None of those were used here. So, the “improves proprioception” claim isn’t what the study showed. What the study showed was improved short term static balance, with eyes closed, while the braid was on. That’s a real finding, but it’s a much smaller one.
A few more, quickly. No functional outcomes, so no gait analysis and no fatigue measure, which means the “returns the spring to your step” line sits on nothing the study measured. No washout period described in a crossover design where washout matters. And roughly ten significance tests with no correction for multiple comparisons. With ten tests at the standard threshold, the chance of at least one false positive by luck alone is around forty percent. Some of those p values would survive a proper correction. Others wouldn’t.
So, that’s the central evidence. A donated product, a single session, balance standing in for proprioception, no follow up, no functional outcomes, no peer review, no washout, no multiple comparison correction, sixteen people. Read it for what it is, which is a small pilot signal, and it’s fine. Read it as proof the product works, which is how it’s sold, and it falls apart.
The evidence the poster leans on for support
Here’s where it gets more interesting. The Miller poster leans on a tape study as the scientific scaffolding for testing the braid in hypermobility. I pulled it, and read it in full, along with the same group’s follow up. Neither is about the Body Braid, neither supports the proprioception claim, and the most relevant one of the two actively undercuts it, while not appearing on the poster at all.
The study the poster actually cites is Tudini and colleagues, 2023 [2]. This was a randomised trial of kinesio tape against a control tape, in twenty nine adults with hEDS, with a forty eight hour follow up, looking at shoulder pain, range of motion and disability. The result the poster doesn’t quite advertise is that there was no significant difference between the experimental kinesio tape and the control tape on any outcome. Both groups did improve in pain and function over the forty eight hours, and the authors are fair about that, they say tape can offer temporary improvements. The point is that the fancy technique was no better than a plain control strip, so whatever you are feeling is most likely a general skin contact and attention effect rather than anything specific to the taping method. There was no true no tape control, which is the standard weakness of tape studies. And critically, it tested tape, not a spiral elastic garment.
Then there’s the follow up, Tudini and colleagues, 2024 [3], from the same group, same population. The poster doesn’t cite this one, which is the curious part, because it’s the more relevant of the two. This is the study that actually measured Active Joint Reposition error, a genuine proprioception measure, the joint matching task I mentioned earlier. Same comparison, kinesio tape against control tape. And the result was no proprioception improvement at any timepoint, in either group. The authors’ own words: they “cannot recommend K-Tape to improve shoulder AJR in people with hEDS.”
So, sit with that for a second. The one study from this group that actually measured proprioception in hEDS found no effect. From a different product. And it’s the one the poster leaves out, while citing the earlier tape paper that didn’t measure proprioception at all. Either way, there’s nothing here that supports the braid’s proprioception claim.
There’s also a compression garment study worth a mention. It’s the closest thing in the whole literature to “a garment helps balance in hEDS.” Benistan and colleagues, 2024 [4], ran a randomised trial in thirty six adults with hEDS over four weeks. They compared physiotherapy plus compression garments against physiotherapy alone. But the garments here were custom medical grade compression suits, leggings, socks and a vest at ten to fifteen millimetres of mercury. That is a different product class entirely. Medical grade graduated compression is a mechanical and physiological intervention that’s quite distinct from a thin elastic spiral wrap. The dose isn’t shared, the skin coverage isn’t shared, the mechanism isn’t shared. You can’t take a signal from one and assume it transfers to the other.
So, the supporting evidence amounts to a tape study that found nothing, and a compression suit study about a different product. The one study that actually measured proprioception in this group, from the same team as the tape paper, found nothing either, and the poster doesn’t even cite it. None of it involves the Body Braid. None of it supports the specific claim being marketed.
The mechanism story is shakier than it sounds
The Body Braid’s narrative is built on Anatomy Trains, Thomas Myers’ model of continuous myofascial chains that the braid is said to load along. It’s a popular framework in manual therapy and yoga teaching. The trouble is that it’s not strongly supported in the biomechanics literature as a load transmission model in living humans. A systematic review of the evidence for myofascial chains found that cadaver work does confirm several of these connections anatomically, the superficial back line and a couple of the functional lines are really there in dissection. What it does not show is that meaningful tension travels along those chains in a living body, in a way a thin elastic wrap could augment. The review’s own conclusion is that the functional relevance in living people is the urgent open question, so the anatomy is real, the load transmission story is the unresolved part [5].
The “returns the spring in your step” framing borrows from elastic energy storage models, the tendon and fascial recoil that powers efficient movement. Those models describe structures like the Achilles tendon and the plantar fascia. They don’t translate to “a thin garment over the torso restores elastic gait.” That’s a marketing extrapolation, not a biomechanics finding.
Proprioception itself is mediated by muscle spindles, Golgi tendon organs, joint capsule receptors and skin mechanoreceptors. A snug garment can genuinely recruit those skin receptors and add a bit of skin level feedback. That’s the most plausible mechanism for any short term balance effect you might feel. It’s also, funnily enough, the exact same mechanism that explains why kinesio tape sometimes feels like it helps and then consistently fails in controlled trials. Skin receptor stimulation is a real input, but it’s a small one, and it doesn’t restore proprioceptive accuracy in connective tissue that was structurally different to begin with [6][7].
What the wider research actually shows
So, where does the real science sit, when it comes to balance and proprioception in this group?
Proprioception is impaired in those with hypermobility and hEDS. That much is consistent across the literature. Hand position estimate precision is impaired [6], knee joint position sense is reduced compared with controls even after you adjust for physical activity [7], and proprioception contributes to functional capacity in this group, alongside strength [8]. So, the deficit the braid is trying to address is real. That part isn’t in question.
The question is what helps. And when it comes to that, here’s the honest league table. Kinesio tape: no effect on proprioception in the one proprioception specific trial [3]. Custom medical grade compression garments: mixed signals on balance, nothing convincing on proprioception specifically, and no replication outside one French research group [4]. Proprioceptive training, the closed chain exercise and balance work and joint position re-education. Here I’ll be careful, because the evidence base isn’t as tidy as people pretend. Proprioception genuinely matters for function in this group, it’s bound up with muscle strength and activity limitations [8], so addressing it is a sensible target. But the exercise trials themselves are modest. The systematic review of therapeutic exercise in joint hypermobility found that people did improve clinically, yet it also concluded there’s no convincing evidence for one specific type of exercise over another, or that exercise beats a control [9]. So, the honest position is this. Active, exercise based approaches that train proprioception and strength have a more plausible and better studied route to lasting functional change than any garment does, but “better studied” is a low bar here, and nobody should oversell it. What they have that the braid doesn’t is trials that actually measured function and improvement over time, rather than a single session with the kit on.
No class of wearable garment, tape, or wrap has produced strong, replicated evidence for sustained proprioceptive improvement, off the garment, in hEDS. None of them. The Body Braid is no exception to that, it’s simply less studied than the alternatives.
And here’s a useful cross check. The Body Braid does not appear in any indexed academic database, not PubMed, not Google Scholar, not Web of Science, outside that single Miller poster. The wider hEDS research community hasn’t engaged with the product at all. It is not on the academic radar, despite being sold as evidence based.
The three things I actually noticed wearing it
Right, so that’s the marketing pulled apart. But I promised you the other half, and this is the part I find genuinely interesting, because it’s not on the box.
Before I get into it, one honest caveat, and I’m only going to say it once. None of what follows is a Body Braid study. There is no Body Braid study for any of this. What I’m describing is the underlying movement and breathing science that explains why a snug, spiralled garment giving you feedback could plausibly help. It’s mechanism, not proof the braid does it. Keep that in your head for the next three sections.
One: it seemed to help my counter-rotation when I walk
When I wore it, the thing I noticed first was my walking. Specifically, the way my ribs and pelvis rotate against each other as I move. It felt smoother, somehow more connected, so I went and looked at whether that’s a real thing in this population.
It is, and the science here is genuinely strong. When you walk normally, your pelvis and your ribcage rotate in opposite directions, and that counter-rotation grows as you speed up. The shift from moving together to counter-rotating is a well established feature of efficient, healthy gait [10].
Now, here’s what chronic pain does to it. People with low back pain show more in phase rotation, which is to say the ribs and pelvis start moving together as a single block instead of counter-rotating [10]. The research reads this as a protective guarding strategy, the system stiffening the trunk to avoid large or fast spinal rotation, and it shows up as higher mechanical coupling between the thorax and pelvis in people with back pain [11]. It even appears in chronic neck pain, where people walk with a stiffer spine and reduced trunk rotation [12]. And keeping everything locked together like that is more energetically demanding, it blunts the natural arm swing, the whole thing gets less efficient.
So, when I say it felt like the braid nudged that opposite direction rotation back in, the reason that’s plausible holds up. This guarded, locked up pattern is well documented in chronic pain states, though the direct hypermobility specific data on trunk rotation is still thin. We don’t have a study showing the braid fixes it. But the mechanism it would be working on is not made up.
Two: it seemed to help pull my leg through
The second thing was leg swing. It felt like the braid was helping my leg swing through during walking, that bit where one leg is in the air travelling forward. So, same question. Is gait actually altered in this group?
Very much so. People with hypermobility and EDS tend to walk with a stiffening pattern. That means shorter steps, longer time with the foot planted, and reduced power generation, which the research reads as a strategy to avoid pain and protect balance [13]. There’s also measurable hip extensor weakness, on the order of a forty percent deficit, and a lower hip extensor moment during walking in hEDS, and the hip drive is exactly what powers you forward and helps advance the limb [14]. Layer on the reduced sense of where the joints are in space [15], and you get a stiffer, more guarded, more effortful walk.
Now, tie that back to the first thing. The trunk counter-rotation and the arm swing are part of what helps drive the opposite leg through. If the trunk is locked up, the free momentum that should help swing the other leg gets blunted. Which fits exactly what I felt the braid restoring. Worn through the day, something that keeps nudging that rhythm could be a useful training cue. But again, that’s a mechanism I’m describing, not a clinical result.
Three: the belly straps gave me 360 degree breathing feedback
This is the one I think is genuinely clever, and it’s the one the marketing misses entirely.
When I breathed in wearing the braid, I could feel the straps across my stomach, my sides and my back. And that’s a much bigger deal than it sounds, because breathing problems are common in this community and most people don’t realise it. Breathlessness affects around half of people with hEDS, and reduced inspiratory muscle strength shows up in around three quarters of them, both figures coming from the same cohort that looked at this [16], with lung volume perception itself measurably impaired in this group [21]. On top of that, there’s a marked increase in respiratory symptoms, including more breathlessness on walking, across EDS and HSD [17].
Pelvic floor problems are common too, and the two are linked, because your diaphragm and your pelvic floor work together like a piston. Breathe in, the diaphragm descends and the pelvic floor lengthens. Breathe out, it recoils. Their motion is correlated [19], and they’re part of one pressurised system that runs from the diaphragm through the abdominal wall to the pelvic floor [20]. Pelvic floor dysfunction, including pelvic organ prolapse, runs well above the general population in this group [18]. When breathing gets stuck in a braced, chest dominant pattern, both ends of that piston suffer.
Part of why this matters is that a big chunk of this community runs on a chronically upregulated nervous system. That means the fast, shallow, chest dominant breathing pattern that tends to come with dysautonomia, and that pattern quietly trains the diaphragm out of doing its proper job. There’s also evidence in low back pain that breathing mechanics and trunk function are coupled, with measurably less diaphragm and pelvic excursion when the trunk is guarded, which is the same kind of guarding this group does. So, the breathing and the movement aren’t separate problems, they’re the same stiffened, braced system showing up at different ends of the body.
So, here’s why the straps matter. Tactile feedback, having something to push against as your ribs and sides and back expand, is a recognised teaching tool for 360 degree breathing. It’s the difference between heaving your chest up and actually breathing into your whole ribcage, and it’s exactly what breathing retraining uses on purpose for people who can’t otherwise feel the movement. A strap sitting across the stomach, sides and back gives precisely that kind of resistance against expansion cue. And this is a population that disproportionately needs it. Population level, that’s a sensible use of a feedback tool. It’s not a treatment, and there’s no braid study on it. It’s a feedback tool doing what feedback tools do.
So, is the Body Braid worth it?
Here’s where I land, and I’ll keep it honest.
A spiral elastic garment may well give some people with hypermobility an immediate, while wearing sense of better balance and a bit less pain. That’s broadly consistent with what we know about skin receptor stimulation and the general garment literature. People will report it feels useful. Some will keep wearing it, and if it genuinely helps you feel more put together through the day, that’s not nothing. When it comes to chronic pain, the felt sense of being more in control of your own body is worth something, even when a lab can’t measure it.
So, let me be clear about where I land on the product, because I genuinely rated it. It’s a good, well made, well designed bit of kit, and plenty of people will get something out of wearing it. As a little training tool and a comfort layer, there’s a lot to like. The problem isn’t the product. The problem is the marketing.
The “evidence based” framing rests on one unpublished sixteen person poster, where the company supplied the kit. Balance was measured instead of proprioception, there was no follow up beyond the testing session, and the supporting tape and garment studies are about different products, while the one study from the same group that did measure proprioception found no benefit and isn’t even cited. The mechanistic story leans on Anatomy Trains, a model that’s popular in manual therapy but not very well supported in the biomechanics. And the wider expert community isn’t citing the Body Braid as a serious intervention at all. So, when it comes to the claim that this is science backed, the science just isn’t there yet.
Anyone selling this to those with hypermobility as scientifically validated for proprioception is overreaching what the data shows. There’s a small, short term comfort and balance signal in a tiny study. That’s the honest summary. Whether that’s worth the price tag to you is a personal call, but at least now you’re making it with the actual evidence in front of you, not the marketing version of it.
And the three things I noticed? They’re real mechanisms with real science behind them. They’re just not the science the box is selling, and they’re not proof the braid delivers them. If you do try one, try it as a feedback tool that might cue better movement and breathing, not as a treatment that fixes your joints. That framing will save you a lot of disappointment.
Related reading
If this was useful, here is where to go next, depending on what you are working on.
- how proprioception and cortical body maps actually work
- why your nervous system learns movement the way it does
- the reason hypermobile muscles can feel tight and weak at once
- what the research really says about fascia
- the honest verdict on compression garments
- whether KT tape does anything it claims
Frequently asked questions
Is the Body Braid scientifically proven to work for hypermobility?
No, and it’s worth being precise about what that means. The absence of published evidence does not mean the product does nothing. It means we don’t yet have the studies to know whether it works, or how well. The only direct evidence is a single unpublished conference poster of sixteen people, measured in one session, with the product donated by the manufacturer [1]. It showed a short term improvement in static balance with the braid on, but it didn’t measure proprioception directly, had no follow up, and hasn’t been peer reviewed or replicated. That’s a pilot signal, not proof.
Does the Body Braid improve proprioception?
The marketing says so, but the study it points to didn’t actually measure proprioception. It measured static balance and self reported pain [1]. Proprioception is measured with specific joint position and motion detection tasks, and none of those were used. Interestingly, the one study from that research group that did measure proprioception in hEDS, using a different product, found no effect, and the poster doesn’t even cite it [3].
Is the Body Braid better than compression garments or exercise?
There’s no head to head evidence, so this can’t be answered directly. What we can say is that proprioception is genuinely bound up with strength and day to day function in this group, so it’s a sensible thing to train [8], and exercise based approaches at least have trials that measured functional improvement over time. The honest caveat is that those exercise trials are modest, and the systematic review found no convincing evidence that one type of exercise beats another or beats a control [9]. So, active training has a better studied route to lasting change than any garment, but it’s a low bar and not a slam dunk. Medical grade compression has a weak, unreplicated signal for balance [4], and that’s a different product to the braid anyway.
Can the Body Braid still feel helpful even if the evidence is weak?
Yes, and this is worth saying plainly. A snug garment can recruit skin receptors and give you tactile feedback, which can genuinely make you feel more aware of your posture, your walking rhythm and your breathing [6][7]. Feeling more put together while you wear something is a real experience. Just be clear that feeling helpful in the moment is different from producing lasting, measurable change off the garment, which is what hasn’t been shown.
Is it safe to try?
For most people a light elastic garment is low risk, but this isn’t medical advice and we can’t tell you what’s right for your body. If you have circulation issues, skin fragility, or any condition where compression or restriction could be a problem, check with a clinician who knows your history first. And if you do try it, think of it as a movement and breathing cue rather than something that treats the underlying condition.
References
- Miller, A.J. et al. (2025) ‘The effect of the Body Braid on balance and pain in individuals with hypermobility’, Lebanon Valley College Department of Physical Therapy research poster. [conference poster, no DOI; BodyBraid product donation disclosed]
- Tudini, F., Levine, D., Healy, M., Jordon, M. and Chui, K. (2023) ‘Evaluating the effects of two different kinesiology taping techniques on shoulder pain and function in patients with hypermobile Ehlers-Danlos syndrome‘, Frontiers in Pain Research, 4. doi:10.3389/fpain.2023.1089748
- Tudini, F., Jordon, M., Levine, D., Healy, M., Cathey, S. and Chui, K. (2024) ‘Evaluating the effects of two different kinesiology taping techniques on shoulder range of motion and proprioception in patients with hypermobile Ehlers-Danlos syndrome’, Frontiers in Rehabilitation Sciences, 5. doi:10.3389/fresc.2024.1383551
- Benistan, K., Foy, M., Gillas, F., Genet, F., Kane, M., Barbot, F., Vaugier, I., Bonnyaud, C. and Gader, N. (2024) ‘Effects of compression garments on balance in hypermobile Ehlers-Danlos syndrome: a randomized controlled trial’, Disability and Rehabilitation, 46(9), pp. 1841-1850. doi:10.1080/09638288.2023.2209742
- Wilke, J., Krause, F., Vogt, L. and Banzer, W. (2016) ‘What is evidence-based about myofascial chains: a systematic review’, Archives of Physical Medicine and Rehabilitation, 97(3), pp. 454-461. doi:10.1016/j.apmr.2015.07.023
- Clayton, H.A., Jones, S.A.H. and Henriques, D.Y.P. (2015) ‘Proprioceptive precision is impaired in Ehlers-Danlos syndrome’, SpringerPlus, 4, p. 323. doi:10.1186/s40064-015-1089-1
- Rombaut, L., De Paepe, A., Malfait, F., Cools, A. and Calders, P. (2010) ‘Joint position sense and vibratory perception sense in patients with Ehlers-Danlos syndrome type III (hypermobility type)’, Clinical Rheumatology, 29(3), pp. 289-295. doi:10.1007/s10067-009-1320-y
- Scheper, M., Rombaut, L., de Vries, J., De Wandele, I., van der Esch, M., Visser, B., Malfait, F., Calders, P. and Engelbert, R. (2017) ‘The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception’, Disability and Rehabilitation, 39(14), pp. 1391-1397. doi:10.1080/09638288.2016.1196396
- Palmer, S., Bailey, S., Barker, L., Barney, L. and Elliott, A. (2014) ‘The effectiveness of therapeutic exercise for joint hypermobility syndrome: a systematic review’, Physiotherapy, 100(3), pp. 220-227.
- Lamoth, C.J.C. et al. (2006) ‘Effects of chronic low back pain on trunk coordination and back muscle activity during walking: changes in motor control’, European Spine Journal, 15(1), pp. 23-40. doi:10.1007/s00586-004-0825-y
- van den Hoorn, W., Bruijn, S.M., Meijer, O.G., Hodges, P.W. and van Dieën, J.H. (2012) ‘Mechanical coupling between transverse plane pelvis and thorax rotations during gait is higher in people with low back pain’, Journal of Biomechanics, 45(2), pp. 342-347. doi:10.1016/j.jbiomech.2011.10.024
- Falla, D., Gizzi, L., Parsa, H., Dieterich, A. and Petzke, F. (2017) ‘People with chronic neck pain walk with a stiffer spine’, Journal of Orthopaedic & Sports Physical Therapy, 47(4), pp. 268-277. doi:10.2519/jospt.2017.6768
- Galli, M., Cimolin, V., Rigoldi, C., Castori, M. et al. (2011) ‘Gait strategy in patients with Ehlers-Danlos syndrome hypermobility type: a kinematic and kinetic evaluation using 3D gait analysis’, Research in Developmental Disabilities, 32(5), pp. 1663-1668. doi:10.1016/j.ridd.2011.02.018
- Ball, L.N. et al. (2024) ‘Assessment of gait mechanics and muscle strength in hypermobile Ehlers-Danlos syndrome’, Clinical Biomechanics, 113, p. 106210. doi:10.1016/j.clinbiomech.2024.106210
- Smith, T.O. et al. (2013) ‘Do people with benign joint hypermobility syndrome (BJHS) have reduced joint proprioception? A systematic review and meta-analysis’, Rheumatology International, 33(11), pp. 2709-2716. doi:10.1007/s00296-013-2790-4
- Reychler, G., Liistro, G., Pierard, G.E., Hermanns-Le, T. and Manicourt, D. (2019) ‘Inspiratory muscle strength training improves lung function in patients with the hypermobile Ehlers-Danlos syndrome: a randomized controlled trial’, American Journal of Medical Genetics Part A, 179(3), pp. 356-364. doi:10.1002/ajmg.a.61016
- Chohan, K. et al. (2021) ‘A review of respiratory manifestations and their management in Ehlers-Danlos syndromes and hypermobility spectrum disorders’, Chronic Respiratory Disease, 18. doi:10.1177/14799731211025313
- Gilliam, E., Hoffman, J.D. and Yeh, G. (2020) ‘Urogenital and pelvic complications in the Ehlers-Danlos syndromes and associated hypermobility spectrum disorders: a scoping review’, Clinical Genetics, 97(1), pp. 168-178. doi:10.1111/cge.13624
- Park, H. and Han, D. (2015) ‘The effect of the correlation between the contraction of the pelvic floor muscles and diaphragmatic motion during breathing’, Journal of Physical Therapy Science, 27(7), pp. 2113-2115. doi:10.1589/jpts.27.2113
- Bordoni, B. and Zanier, E. (2013) ‘Anatomic connections of the diaphragm: influence of respiration on the body system’, Journal of Multidisciplinary Healthcare, 6, pp. 281-291. doi:10.2147/jmdh.s45443
- Hakimi, A., Bergoin, C., De Jesus, A., Hermand, E., Fabre, C. and Mucci, P. (2024) ‘Impairment of lung volume perception and breathing control in hypermobile Ehlers-Danlos syndrome’, Scientific Reports, 14, p. 8019. doi:10.1038/s41598-024-58890-2