If you’ve got hypermobility, somewhere along the way someone has probably told you your proprioception is bad. Maybe a physio. Maybe a PT. Maybe the YouTube algorithm. And then the conversation moved on, because nobody really explained what proprioception is, why yours might be off, what the brain has to do with it, or what you’re supposed to actually do about it. So you ended up doing wobble board work on a Tuesday and assuming that was the fix.
Add a metabolic or hormonal layer like PCOS (renamed PMOS in 2026) and the prescription needs further tailoring. The cardiometabolic returns of resistance training are the same, but the implementation has to respect both hypermobility and the metabolic picture. Full breakdown in PCOS to PMOS and hypermobility.
In Part 1 of this two part piece, we argued that the strength training model for hypermobility falls short because muscle output is downstream of a sensory and motor learning problem. This piece picks up the other end of that argument. What is proprioception, really. Why does it go wrong in hypermobility, when it does. What is the brain doing with the signal once it gets there. And, because the question gets asked a lot, has the old “chronic pain smudges your brain map” story actually held up since 2019? The short answer to that last one is: not quite the way we used to tell it.
This is going to be a longer read. It earns its length because the field has moved, the older confident claims about cortical reorganisation in chronic pain have been revisited under better scanners, and the practical implications for those with hypermobility are not what most rehab guidance still says they are. If you want the bottom line up front: yes proprioception is worse in symptomatic hypermobility, no it isn’t worse just because you’re hypermobile, and the brain side of the story is more interesting and more honest than the marketing version.
What Proprioception Actually Is
Strip it back. Proprioception is the sense of where bits of you are without looking. Close your eyes and bring your finger to your nose. The fact that you can do that, more or less, is proprioception working. It’s built out of three things, blended in real time with what your eyes and inner ear are telling you. Joint position sense, which is the static “where is my knee right now” piece. Kinaesthesia, which is the moving “my knee is bending and at this speed” piece. And force sense, which is the “how much effort am I currently putting through it” piece [13, 2, 3].
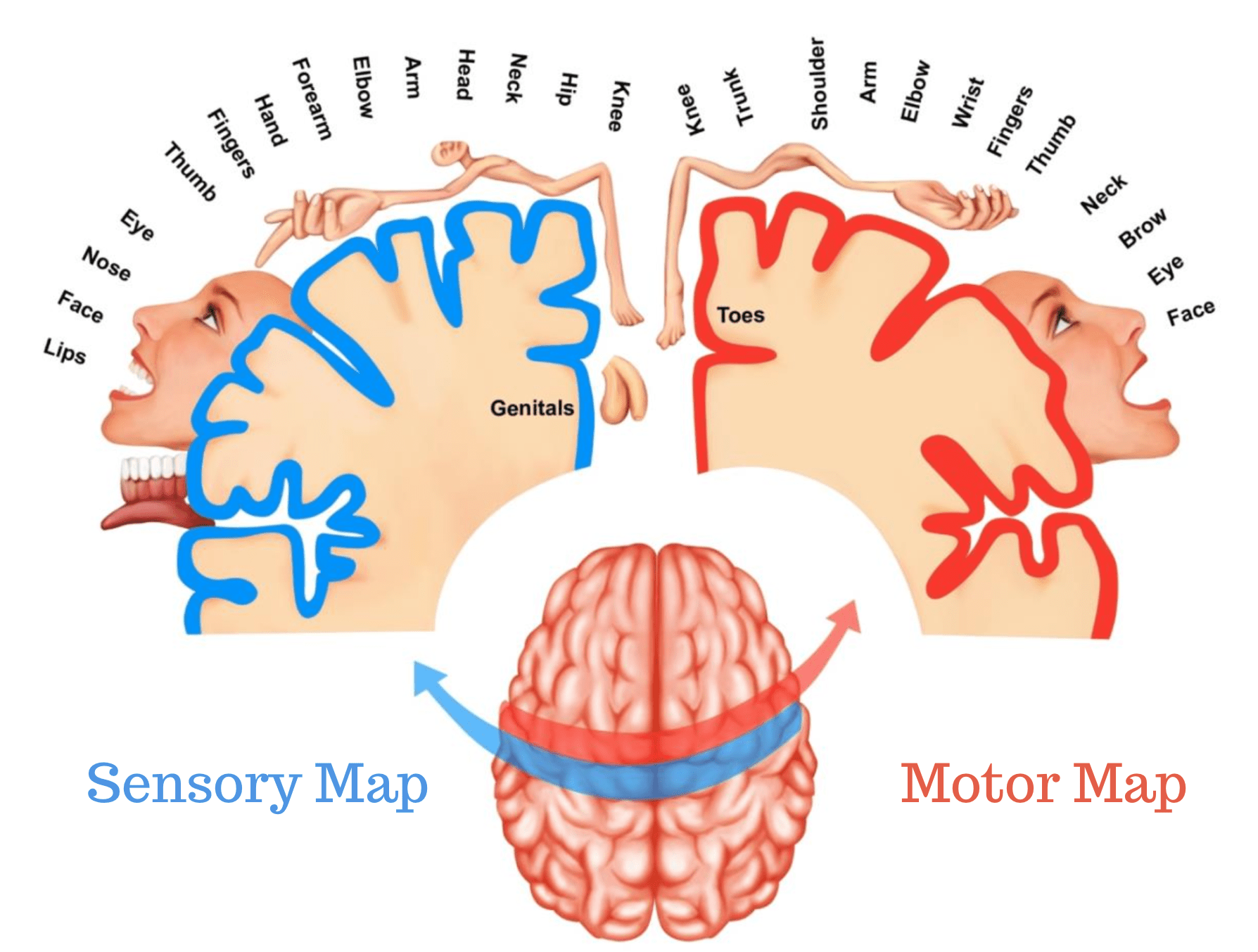
The signal itself comes from a few places. Muscle spindles inside the muscle. Golgi tendon organs at the tendon. Joint capsule receptors. Skin mechanoreceptors at the surface. All of those feed up to the spinal cord, up to the brainstem, up to thalamus, and finally to the primary somatosensory cortex (S1) where they get laid out on a body map. There’s a more useful way to think about it though. The brain isn’t sitting back waiting for the signal to arrive and reading it off like a screen. It’s predicting where you should be, comparing the prediction to the signal, and adjusting in real time. Moseley, Gallace and Spence called this the cortical body matrix, and the framing helps a lot, because it puts proprioception inside an active forecasting system rather than treating it as a passive readout [20].
Why does that matter? Because if the prediction is off, or the signal is fuzzy, or both, the motor system gets fed bad numbers and the movement comes out wrong. You don’t get a tidy “no signal” warning. You get a knee that buckles a fraction late, a shoulder that rolls a few degrees further than you meant, a foot that lands on the wrong bit of the cobble. The system papers over the gaps. It just papers over them by relying more heavily on vision, or by bracing, or by reducing the range of movement until things feel safe again. We’ll come back to all three.
Is Proprioception Really Worse In Hypermobility?
When it comes to proprioception in hypermobility, this is the question that needs a careful answer, because the loose version (hypermobile = bad proprioception) doesn’t hold up under the recent evidence, and getting it wrong has real consequences for what you train.
In symptomatic adults, the picture is fairly clear. Joint position sense is worse at the shoulder and knee in those with the hypermobility syndrome [1, 2]. It’s worse at the finger interphalangeal joint [4]. A 2025 study in adults found higher Beighton scores were associated with greater joint position errors at both elbow and knee, with a dose response pattern that didn’t show up cleanly in earlier work [5, 8]. Lumbar proprioception is in the same place, with errors a few degrees larger than controls [14]. Vibratory perception is reduced at the medial malleolus in adults with the hypermobility type of Ehlers-Danlos, which is the sort of finding that hints at large fibre involvement, not just lax joint capsules [1].
Then there’s kinaesthesia. Adult women with hEDS showed roughly forty four per cent greater movement detection error than controls in one study, meaning the threshold at which they could detect their limb starting to move was higher [9]. Children with the hypermobility syndrome showed both worse joint position matching and worse kinaesthesia at the knee, plus reduced quadriceps torque on isokinetic testing [3]. Clayton and colleagues, looking at hand position with only afferent information available, found EDS adults were as accurate as controls on average but showed roughly double the scatter [13]. Accurate but imprecise. That distinction matters. They can find their thumb. They just can’t find it twice in the same spot.
Now here’s the bit that gets glossed over. Asymptomatic generalised joint hypermobility, the kind a child has when they can do the Beighton tricks but isn’t in pain, doesn’t reliably show the same proprioceptive deficits. Ituen and Smits-Engelsman, in a 2024 study of 150 children, found no impairment in proprioception or its relationship with range of motion in hypermobile versus normally mobile kids [6]. A separate 2024 study from the same group in 588 children compared dynamic balance and strength and again found the hypermobile group was not consistently worse [7]. Read those alongside the adult findings and the picture isn’t “hypermobile means bad proprioception”. It’s that proprioceptive impairment tracks with symptomatic presentation, not with a positive Beighton score on its own. The Beighton, useful as it is, doesn’t tell you whether the nervous system is also affected.
So the honest answer, when it comes to whether your proprioception is worse, is: if you have hEDS or HSD with pain, instability, falls, or trouble grading effort, then probably yes. If you’re hypermobile and asymptomatic, probably not in any clinically meaningful way. Which is also why the worried mum on Facebook whose kid scores nine out of nine on the Beighton but is otherwise fine doesn’t necessarily need to drag the kid to a balance class. Symptoms first. Score second.
What does symptomatic instability look like joint by joint? It depends where the problem lives. We’ve covered the specifics in the pieces on hypermobile knees and on wrist pain. The very confusing presentation of being hypermobile but not flexible is a separate piece worth a look. And allodynia can be in the mix too, which complicates the read.
Why Does It Happen In The First Place?
The old story goes something like: joints are loose, joint receptors fire weirdly, brain gets bad information. That’s partially true and very incomplete. The more interesting work, when you actually look into the mechanism, points somewhere a bit different.
Long and Alexander’s 2022 case control study did the kind of thing rehab researchers should do more of. They didn’t just measure the output. They went looking for where in the nervous system the problem actually sits. They used transcranial magnetic stimulation to measure corticospinal excitability and the H reflex to look at spinal reflex arcs. In symptomatic hypermobile adults, corticospinal excitability was actually steeper, not weaker, than in controls. The H reflex was unchanged. Read that for a second. The brain is sending more drive down the cord, not less. The reflex loop is normal. So the bottleneck isn’t sitting in central pathways and it isn’t sitting in the spinal cord [12].
Where does that leave the deficit? Peripherally, most likely. At the receptors themselves and at the tissue they sit in. Muscle spindles don’t fire in a vacuum. They fire based on the length and rate of change of the muscle they sit inside, and that’s modulated by how taut the surrounding tissue is. If the connective tissue housing is laxer, the mechanical signal that reaches the spindle is different. The brain gets a noisier, less reliable read, even though the brain itself is firing on all cylinders. That’s a different problem to “your brain map is wrong”. It’s a “the input is degraded before it ever gets uploaded” problem. The implication is direct. Tightening up the housing, by building muscle tone in the right way, isn’t a metaphor. It’s a sensible mechanical intervention on the signal pathway [12]. We’ve gone deeper on the tone side of that argument in our piece on hypermobile muscle tone, and on the connective tissue side in the pieces on fascia and on whether hypermobile bodies really have less collagen.
There’s a wider angle worth a quick mention. Predictive coding models of interoception, the way the brain forecasts internal body signals, suggest that imprecise proprioception means the prediction error stays large, the system runs hot, and downstream effects on autonomic regulation and emotion can follow. That’s part of why anxiety in hypermobility often isn’t just “psychological” in the dismissive sense, and why fear of movement shows up so reliably. The system is being asked to act on noisy data. Acting on noisy data is anxiety provoking, regardless of which species you are.
Falls, Balance And The Vision Crutch
Once proprioception is fuzzy, the brain doesn’t just throw its hands up. It reweights. The vestibular system, which tells you which way is down, gets used more. Vision gets used a lot more. And what you end up with is a person who looks fine when their eyes are open on a stable surface, and falls apart the moment either of those things change. Co contraction of muscles can occur, and active muscle tone can increase to take up the reduce passive tone: it’s a big contributing factor in why you always feel tight, and can never seem to relax.
The numbers are striking. Rombaut and colleagues followed women with hEDS for a year using a fall diary and found roughly ninety five per cent reported at least one fall over the twelve months. Postural sway velocity and area were greater than in controls [10]. Whitmore’s 2023 work using a wearable balance system found that sway on foam with eyes closed was roughly two to three times that of healthy controls in hEDS [15]. Open your eyes back up, put your feet on solid ground, and the difference shrinks. Take both away and the deficit shows itself.
A 2025 study in hypermobility syndrome by ALMohiza pulled this together. Limits of stability were about eighteen per cent lower than controls. Lumbar joint position errors were one to three degrees larger. Kinesiophobia and fatigue partially mediated the relationship between proprioception and stability [14]. So it isn’t just “bad balance because bad receptors”. The fear of moving, the energy state, the willingness to risk going to the edge of the supporting base, all of that’s stitched into the result. You can’t separate the proprioceptive signal from the person carrying it around all day, which is part of why pacing the load you put through the system ends up mattering as much as the drills.
The vision over reliance is well documented. Dupuy’s 2017 work using somatosensory orthoses (compression garments, textured insoles) in hEDS showed that giving the body better cutaneous input reduced postural sway, especially with the eyes closed [11]. That’s a clue. The skin can be recruited to substitute for impaired joint receptors. The compression garment isn’t doing structural work. It’s giving the nervous system more channels to listen to. KT tape lands in the same space, and we’ve written about how that’s better understood as a sensory tool than a mechanical one.
So when somebody closes their eyes during a balance test and suddenly the system falls over, that isn’t failure. It’s the system showing you where the proprioceptive signal was thin all along. The vision had been quietly papering over the gap. Take it away and the gap appears. Which is also why foot work matters so much in this population. The foot is a huge skin and joint sensor array, and most people are walking around in cushioned shoes that mute it.
The Brain Map Story, And Why 2019 Changed It
Now, when it comes to the brain side of all this, this is the section that’s been sitting at the back of every modern pain rehab conversation for fifteen years, and it’s the one most likely to be told confidently and wrong. The short version of the popular story goes like this: chronic pain “smudges” your brain map, the bit of the somatosensory cortex that represents the painful body part loses resolution and blurs into neighbouring areas, and rehab needs to “rewire” or “redraw” the map to reduce pain. You’ll have heard it on Instagram, on YouTube, in pain management programmes, and from some clinicians. It’s confident. It’s catchy. It also, since around 2019, hasn’t quite held up under the better scanners.
Where did the story come from? Flor and colleagues, 1995, in Nature. Using magnetoencephalography (MEG), they showed that the magnitude of phantom limb pain after amputation correlated with the degree of cortical reorganisation in S1, with the face area appearing to invade the former hand area [19]. That was the seed. Through the 2000s the framework expanded. Moseley and Flor’s 2012 review in Neurorehabilitation and Neural Repair put it into rehab language. Target the cortical representations. Sensory discrimination training. Mirror therapy. Graded motor imagery. The argument was that if the cortex had reorganised maladaptively, the rehab job was to coax it back [21]. Schabrun and colleagues showed similar smudging in motor cortex in low back pain, with the disorganisation correlated to pain severity [22]. Catley’s 2014 meta-analysis pulled together twenty six studies suggesting tactile acuity is impaired in chronic pain across multiple conditions [23]. So far so consistent.
Then Mancini, with Moseley as a co-author, ran the experiment the field had been needing. 2019, in the Journal of Neuroscience. Eighteen people with chronic complex regional pain syndrome (CRPS) and seventeen controls. 3 Tesla MRI at a spatial resolution of one and a half cubic millimetres. Fine grained, finger by finger mapping of S1. If the smudging story was right, the affected hand’s representation should have been visibly degraded. It wasn’t. Map area, location and geometry were “largely comparable” to controls. The paper’s own conclusion, in the abstract, is worth quoting directly: the findings “compel us to reconsider the cortical mechanisms underlying CRPS and the rationale for interventions that aim to ‘restore’ somatotopic representations to treat pain” [16].
Two things to flag. First, Moseley was on that paper. The person whose 2012 review crystallised the smudging framework was a co-author of the paper showing the framework needed reconsidering. That’s how science is supposed to work. Second, this wasn’t an isolated finding. The phantom limb literature was moving the same way.
Makin and colleagues, 2013, in Nature Communications, showed that chronic phantom limb pain was positively associated with maintained, not degraded, cortical hand representation. The former hand area was active when the person tried to move their phantom, and the level of activity tracked with the pain. That doesn’t fit a smudging model. It fits a preserved representation model [17]. A 2015 follow up replicated this [25]. Kikkert’s pre-registered 2018 replication confirmed it again, with the statistical evidence favouring the maintained representation model over the maladaptive plasticity model [26]. Then in 2025, Schone, Makin and colleagues did something nobody had done before. They scanned three adults longitudinally, before and after planned arm amputation, with fMRI. Cortical body maps were stable. Their wording was clear: amputation does not trigger large scale cortical reorganisation [27].
Makin and Flor co-authored a 2020 reconsideration in NeuroImage, explicitly arguing the field needed to look beyond S1 remapping and into broader sensorimotor, contextual, and emotional mechanisms [28]. That’s not throwing out everything that came before. That’s saying the explanation we’d been using was too simple and the cleaner data points elsewhere. Makin and Bensmaia, in a 2017 Trends in Cognitive Sciences piece, had already laid the groundwork for that reconsideration, arguing that sensory topographies in adult cortex are more stable than the older plasticity models implied [18]. The 2023 work by Hotta added a useful detail. Functional connectivity within sensorimotor cortex in CRPS can be disrupted even when the gross somatotopic maps look intact [24]. So something is going on in the wiring between regions, even if the regions themselves haven’t slid around.
Worth dropping in one more piece of work, because it cuts a popular assumption. Mancini’s 2014 study in Annals of Neurology mapped spatial acuity for pain and for touch across the whole body. They follow opposite gradients. And in a patient with no functioning large fibre touch input, pain acuity was preserved. Pain and touch are neurally dissociated [30]. That matters because the tactile acuity training argument (two point discrimination, sensory drills) was built partly on the assumption that touch and pain ride together. The 2014 data say they don’t.

Ready to work through this with structure and support?
The Hypermobility Live Workshop is four weeks of breaking down the frameworks we use in our studios, with live Q&A so you can ask about your specific situation. Two free courses are included.
What does any of that mean for hypermobility specifically? Honestly, here’s the gap. There is no published fMRI or MEG study of S1 or S2 body map organisation in hEDS or HSD. None. Not a single high resolution cortical mapping study in this population as of 2025. A 2025 clinical study did go looking for somatognosia and stereognosis deficits in hypermobile people and found no significant link with hypermobility scores [29]. So the central body schema, at least at that level of measurement, doesn’t appear to be the problem either. Which puts us back where Long and Alexander put us. The signal is most likely degraded peripherally, the brain is doing its best with what it’s getting, and there’s no good evidence the maps themselves are smudged in this population. We’ve written more about the cortical mapping work in adjacent conditions in the Parsonage Turner brain sensory mapping piece, and on broader cortical thickness differences in the ASD and ADHD cortical thickness piece.
The honest framing, then. Smudging hasn’t been falsified. M1 smudging in low back pain looks real [22]. S1 smudging in CRPS, when looked at with proper resolution, doesn’t [16]. The magnitude in the broader chronic pain field is smaller than the popular story made it sound, the causal direction (pain causes smudging, or smudging causes pain, or some third factor causes both) is genuinely unclear, and in hypermobility it has never been measured. So if anyone tells you confidently that your chronic pain has rewritten your brain maps and your rehab plan is going to redraw them, ask them politely what evidence they’re drawing on. We’ve written more on the actual current models of chronic pain and on hyperalgesia in the relevant pieces.
If The Smudging Story Doesn’t Hold, Why Does Sensorimotor Training Help?
Fair question. Because it does help. The drills work. People feel better. The trials show improvement. The story we’ve been telling about the mechanism is the bit that needs an update, not the practice itself. We have hundreds of clients both in person and online that will attest to that, so whats going on?
The RESOLVE trial, Bagg and Moseley and colleagues in JAMA 2022, randomised 276 adults with chronic low back pain to graded sensorimotor retraining versus a sham control. The active group improved by about one point on the numeric rating scale at eighteen weeks. Statistically clean, clinically modest but real [31]. Then Cashin and colleagues, in Pain 2023, did the mediation analysis on that same trial. The question they asked was: what was actually doing the work? The biggest mediators were psychosocial. Beliefs about back pain, catastrophising, self efficacy. Tactile acuity didn’t mediate the effect. The “sensory remapping” story you might have expected to find as the active ingredient wasn’t there [32]. The active ingredient was how people thought about their pain and their body.
Malfliet’s 2018 trial in JAMA Neurology found that pain neuroscience education combined with cognition targeted motor control beat best evidence physiotherapy in chronic spinal pain, with no detectable change in grey matter volume on MRI [33]. Graded motor imagery and mirror therapy for CRPS do reduce pain and swelling in pooled trials [34], but the cleaner mechanistic read, in light of the imaging work, is that the benefit runs through expectation, attention, reduced fear, and graded re-exposure to the painful body part, rather than through measurable S1 remapping.
So here’s the honest synthesis. The drills are fine. Sensory discrimination training, mirror therapy, graded exposure, tactile cueing, balance work, all of it has a place. What changes is the explanation, we’re reducing threat, rebuilding confidence in moving the painful part, improving the precision of the motor commands going out, and giving the system cleaner sensory information to work with. That’s a less exciting story for marketing. It’s a more durable one for practice. And it stops people getting sold rehab packages on the promise of “neuroplastic rewiring” they can’t deliver and the evidence doesn’t support.
How Proprioception Actually Retrains, The Motor Learning Side
This is the bit that connects directly back to the motor learning piece, so we’ll keep it tight here and skip the foundational stuff covered in Part 1.
Motor learning isn’t strength training. It’s the incremental improvement in selecting and executing actions through practice [35]. Two things matter for our purposes. First, attentional focus. Second, specificity and dose.
Wulf and Lewthwaite’s OPTIMAL theory pulled together two decades of work showing that external focus of attention, where you focus on the effect of the movement (push the floor away, the dumbbell goes up, the ball goes there), beats internal focus on the body part (squeeze the quad, brace the core, tighten the glute) for motor performance, retention and transfer [36]. Chua and colleagues’ 2021 meta-analysis, with 1,824 participants across the literature, confirmed it cleanly. Hedges’ g around 0.26 for performance, 0.58 for transfer, 0.83 for EMG efficiency. The effect held across ages, skill levels, healthy and clinical populations [37]. That’s about as boringly solid a finding as motor control gets. In practice, in studios, the translation is direct. “Push the floor away” beats “tighten your glute”. “The dumbbell goes up to the ceiling” beats “engage your shoulder”. Anything that puts the attention on the muscle as a thing to manipulate makes the movement worse. Anything that puts the attention on the outcome makes it better.
Then specificity. Seo and colleagues’ 2023 systematic review on proprioception training is the cleanest read on this for our population. Targeted proprioception training (deliberately working on joint position sense, kinaesthesia, or force sense with progressive challenge) produced large effects, with Hedges’ g of around 0.75 to 1.18. Non targeted training (general exercise or strength work without a proprioceptive focus) produced medium effects, g of around 0.38 to 0.72. At one week or more of retention, the targeted effect was still around 0.88. The acquisition curve had two time constants. Fast early gains in the first weeks. Slower refinement after. That matches what hypermobile clients actually feel. The first month feels huge. Then it slows. That’s not the programme failing. That’s the second phase of the curve [38].
One sobering bit from the same review. Specificity is real. Joint position sense at the knee trains joint position sense at the knee. It does not magically migrate to the shoulder. So if your shoulder needs work, your shoulder needs work. The wobble board under your foot is not paying that bill [38]. This is also why “core stability training” doesn’t generalise to the whole body in the tidy way some programmes imply.
Tactile Cues, Surfaces, Vision, Dual Tasks
This is the actionable bit. When it comes to what proprioception training actually looks like when it’s built around the research instead of around generic balance class drills, it splits into four overlapping categories.
Tactile cues first. The skin is a sensor array, and in hypermobility, with joint receptors firing imprecisely, the cutaneous channel is one of the cleanest ways to feed the nervous system better positional information. Vibrotactile feedback on the trunk reduces postural sway during walking in vestibular impaired populations [39]. In hEDS specifically, compression garments and textured insoles measurably reduce sway, with the biggest improvements when the eyes are closed and the system has to lean on somatosensation [11]. A hand on the skin during an exercise (a coach’s palm on your low back during a lunge, a band across the thigh during a squat) does the same thing. It thickens the signal. The brain can then drive the muscle more accurately because it has a better read on where the joint is.

Two useful nuances. Anctil and colleagues, 2022, showed that intermittent vibrotactile feedback at thirty three per cent of the time works as well as continuous feedback for balance, with carry over after the feedback is removed [40]. Faded feedback works. You don’t have to have the band on for ever. The whole point is to use the cue to give the system a clearer reference, then take it away as the system internalises the pattern. KT tape, compression sleeves, hand cues, textured floors, all of those sit in the same category. Sensory cleaners, not mechanical splints.
Surface manipulation next. Foam, BOSU, unstable surfaces are not magic, and they’re not for everyone all the time, but they have a real effect when used as part of a targeted programme, especially when trying to work on readiness tone and movement variability, as we looked at in part 1. De Vasconcelos’s 2018 meta-analysis on proprioceptive training in athletes found a thirty eight per cent reduction in ankle sprain incidence in trained groups versus controls [41]. The mechanism, at least the proposed one, mixes spinal reflex modulation with supraspinal adaptation and improvements in rate of force development. Practically, if your ankles are unreliable, surface work has the best evidence base of any single proprioceptive intervention. Pair that with the internal tibial rotation work and the foot arch drills and you’ve got a stack of things to do that all push in the same direction.
Vision restriction next. Because hEDS over relies on vision, eyes closed work is one of the most useful, and most uncomfortable, things you can do. Mechanism, sensory reweighting. Take the dominant input away, force the system to lean on the under used inputs, and over time those inputs get better used [11, 38]. Practical rule, start with eyes closed on a stable surface. Standing on two feet. Then one. Then a soft surface. Don’t combine eyes closed with an unstable surface on week one. The point is to challenge the system, not to launch it across the kitchen. Sensible progression matters more in hypermobility than in most other populations, because the failure mode isn’t “doesn’t get strong”. It’s “tips over and gets hurt”.
Dual tasking. Once a movement has been practised enough to be roughly automatic, adding a cognitive load on top is one of the better ways to push it the rest of the way to automaticity. Stand on one leg while counting backwards from one hundred. Walk while doing a simple recall task. Hold a tandem stance while tracking a moving object. Chiaramonte’s 2022 review showed dual task and proprioceptive training together drove improvements in stroke rehabilitation that single mode training didn’t match, and the principle generalises [42]. You don’t need a stroke to use the principle. You need a movement you can do at maybe seventy per cent attention, then you steal twenty per cent of that attention with something cognitive, and you let the motor system find a way.
Strength as infrastructure. This loops back to the spindle housing argument [12]. Strength work isn’t a substitute for proprioceptive work, it’s the structure that proprioception sits inside. Higo and colleagues’ 2024 systematic review found that high load shoulder strengthening in hEDS produced large effects on shoulder function and pain [43]. That’s not a fluke. That’s strength rebuilding the mechanical context that the receptors work in. Strength and proprioception aren’t competing approaches. They’re layered. Trunk and core work belongs in the same conversation, and so does running once the system is ready for it. Joint specific work, including for ribs, spinal asymmetries, and the jaw, follows the same pattern. Specific sensor, specific drill, build the mechanical context around it.
A Staged Way To Think About It
This isn’t a strict three step ladder, because the stages overlap in real life, but it’s a useful way to think about what gets weighted when.
Stage one, awareness. Slow, low load, plenty of feedback. The goal here is to feel where you are. Single leg stance with a hand on the wall. Sit to stand with an external focus cue (push the floor, not squeeze the glutes). Hand on the thigh during a hinge. Easy work, deliberately. The aim isn’t to fatigue the system. The aim is to give it a chance to notice itself [44, 45].
Stage two, variability. Same fundamental actions, with the variables changing. Different surfaces. Different positions. Different speeds. Different ranges. This is where the schema, in the Schmidt sense covered in Part 1, gets built. The brain is building a rule it can apply across contexts, not a copy of one specific context [38]. Eyes optional. Tactile cues optional. External focus throughout.
Stage three, load and automaticity. Strength gets added in earnest. Dual tasks come in. Sport or life specific demands start being practised. The work gets heavier, more complex, and closer to what real life asks of the body [43, 46]. The earlier stages don’t get dropped. They get layered under.
The thing this isn’t is “core first, then everything else”. You don’t earn the right to lift heavy by passing a balance test. The stages run in parallel from week one. The weighting changes over time. Early on, more awareness and variability work. Later on, more load and automaticity, but with the awareness and variability layers still present in the warm up, the cool down, and the more complex drills.
What About Kids?
Quickly, because this is one of the most asked questions in the inbox. Asymptomatic hypermobile children, in the recent studies of 150 and 588 kids respectively, don’t show consistent proprioceptive impairment versus normally mobile peers [6, 7]. Symptomatic children with the hypermobility syndrome, the ones with pain, instability, fatigue, do show worse joint position sense, worse kinaesthesia and reduced muscle torque [3]. The implication is direct. Screen and intervene based on symptoms, not based on a Beighton score in isolation. A hypermobile nine year old who’s fine probably is fine. A hypermobile nine year old who’s falling, in pain, or avoiding play probably needs proper assessment and a properly built programme. We’ve covered the paediatric hypermobility piece separately, and the principles in this article translate to younger bodies in a slightly different dose. And, if I am being totally honest with you, children and pre teens seem to do respond incredibly quickly to target, proper, sensori-motor rehab. Why is this? Well there is potentially more reasons than you can shake a stick at. Most likely, puberty hasn’t kicked in fully, periods haven’t started yet, and kids are just hard wired to learn things quickly.
Take one of pre-teen clients “Berrie” from a few years ago. She was, for lack of better word “Bad” especially in the mobility sense. But, being young and adaptable, she made some absolutely insane progress, fairly quickly, when the right right approach is taking, and you properly educate and apply motor leaning principals.
Honesty About The Evidence
This bit’s important because when it comes to evidence honesty, we’re trying to do the opposite of what most of the rehab content space does. RCT evidence for sensorimotor and proprioceptive training specifically in hEDS and HSD is thin, like the rest of the research when it comes to hypermobility. Most of what we know comes from observational work, small uncontrolled studies, scoping reviews and systematic reviews flagging the lack of high quality trials [44, 46]. The mechanistic work on which our argument leans is from adjacent conditions (CRPS, low back pain, phantom limb) and from the basic neuroscience of motor learning and somatosensation. We don’t yet have a single cortical body map imaging study in hEDS [29]. The most defensible read of the field is that the principles transfer, the targeted drills work better than non targeted ones.
The conservative read isn’t “don’t bother”. It’s: do the drills, use external focus, treat the symptoms not the Beighton, layer strength in as the infrastructure, and stop overselling neuroplasticity. The work is real. The marketing is the bit that needs cleaning up, when it comes to rehab, and the abundance of instagram coaches.
If you haven’t already, Part 1 sets up the why behind all of this, and we’ve also written more specifically about the motor learning principles that drive it. If you want the whole thing run with proper assessment, that’s what our work at the studios and online courses are built for.
If your proprioception, balance and joint control have all been quietly drifting and you’ve been told “just do more balance work” without anyone explaining why, that’s the gap this piece was written to close. The drills are useful. The explanation has changed. And the right way to train this stuff in a hypermobile body looks a fair bit different to what most generic rehab plans put on offer.

The Hypermobility Fundamentals Bundle
The Hypermobility Fundamentals Bundle is a structured education and movement pathway that starts at the bottom and builds upwards, grounded in motor learning and sensory motor science. Designed for people with hypermobility and persistent pain, it focuses on how strength and stability are organised and learned by the nervous system, beginning with the feet and progressing through sensory input, coordination, and motor learning. The courses are intended to be completed in sequence, with each one establishing the concepts and skills needed for the next.
— The Fibro Guy Team —


