
Last updated March 2026
You’ve probably been told to exercise. Maybe by your GP, your physio, or a well-meaning friend who did a half-marathon once. And somewhere in the back of your mind, part of you agrees. You know exercise is supposed to help. But every time you push a little harder, you pay for it. You flare, you crash, you are back on the sofa wondering whether movement is actually making things worse.
This is one of the central tensions in hypermobility management. Movement is medicine, but the wrong kind of movement, done at the wrong intensity, in the wrong sequence, can genuinely make things worse. That is not in your head. It is biomechanics, neuroscience, and connective tissue biology all colliding at once.
This is your starting point. We have pulled together everything you need to know about exercising safely with hypermobility into one place. Each section expands when you click it, and links to a deeper article if you want the full picture. Follow what is relevant to you.
Why Exercise Is Different When You’re Hypermobile

For most people, exercise is fairly straightforward. Load the muscles, stress the system, recover, adapt. With hypermobility, that model breaks. The receptors that should tell your brain where your joints are aren’t firing accurately, joints can travel into ranges your muscles aren’t prepared to catch, and the nervous system itself can be amplified. Here is why standard exercise advice often misses.
Read MoreFor most people, exercise is fairly straightforward. Load the muscles, stress the system, recover, adapt. The body is robust enough to handle a reasonable amount of trial and error. When it comes to hypermobility, this model breaks down in several key ways.
The Proprioception Problem
Proprioception is your body’s ability to sense where its joints are in space. In most people, the mechanoreceptors embedded in ligaments, tendons, and joint capsules send constant positional data to the brain. In those with hypermobility, this system is compromised. The collagen that makes up connective tissue is structurally different, which means the receptors sitting within that tissue don’t fire accurately [1].
A 2022 study investigating quadriceps control in people with symptomatic hypermobility found that the proprioceptive deficit isn’t driven by central nervous system changes, but appears to originate in the connective tissue itself, suggesting that “treatment aimed at improving receptor responsiveness through increasing muscle tone may be an effective rehabilitation strategy” [1]. In practical terms, this means your joints don’t always know where they are. You can hyperextend a knee or dorsiflex an ankle past a safe range without the usual sensory warning that you’re approaching the end of range.
A 2025 study confirmed that people with hypermobility syndrome showed significantly higher lumbar proprioception errors and reduced limits of stability compared to controls, with kinesiophobia and fatigue acting as mediating factors in this relationship [2]. The joints don’t just feel unstable, they are less accurately sensed.
Joint Laxity and the Stability Challenge
Hypermobile joints move beyond the normal physiological range. The passive stabilisers, the ligaments and joint capsules, don’t provide the bracing action they do in more typical connective tissue. This shifts the stabilisation burden entirely onto the active system: the muscles. When those muscles fatigue, or aren’t conditioned enough to provide adequate support, joints can load in uncontrolled positions.
This is why someone with hypermobility can have a knee that looks fine on MRI but still dislocates doing something as mundane as turning over in bed. The imaging shows the structure. It can’t show the dynamic instability that happens when the neuromuscular system fails to keep pace with demand.
Central Sensitisation
Many people with hypermobile EDS (hEDS) and hypermobility spectrum disorders (HSD) also develop central sensitisation, a state in which the nervous system becomes amplified in its pain processing. Studies have found signs of central sensitisation, including exercise-induced hyperalgesia rather than the normal exercise-induced hypoalgesia, in adolescents with HSD/hEDS [3]. This matters a great deal for exercise prescription. In a sensitised system, exercise that would normally feel manageable can produce disproportionate pain responses, which then reinforces fear and avoidance behaviour.
A 2024 study published in European Journal of Pain found signs of central sensitisation in adolescents with HSD/hEDS, including altered conditioned pain modulation and heightened secondary hyperalgesia [3]. This isn’t weakness. It’s a measurable neurological change that needs to be factored into rehabilitation from the start.
Delayed Onset Muscle Soreness: It Hits Harder
Research published in the International Journal of Sports Physical Therapy in 2024 found that people with joint hypermobility syndrome reported significantly higher VAS pain scores following eccentric exercise on Day 2 (p=0.005) and Day 4 (p=0.037) compared to non-hypermobile controls [4]. Both groups experienced DOMS, but the hypermobile group perceived it as considerably more intense. Therapists and individuals with hypermobility both need to factor this in when programming exercise. Longer recovery windows between sessions isn’t a sign of weakness. It’s physiologically appropriate. For more on this, see our guide to core exercises for hypermobility.
Fear of Movement: The Biggest Barrier

If your body has repeatedly hurt you doing ordinary things, caution is not irrational, it is learned. The problem is when caution becomes so pervasive that it blocks the rehabilitation that would actually make movement safer. Kinesiophobia is one of the strongest predictors of how much somebody with hypermobility moves day to day, and tackling it directly is non-negotiable.
Read MoreKinesiophobia, the fear of movement or re-injury, is extremely common in people with hypermobility. And it’s worth being clear: this isn’t an irrational response. It’s a learned one. When your body has hurt you repeatedly in ordinary situations, whether that’s a shoulder subluxation reaching for a glass or a knee giving way on the stairs, caution is a rational adaptation. The problem is when that caution becomes so pervasive that it prevents the very rehabilitation that would make movement safer.
Research consistently shows elevated kinesiophobia in hypermobility populations. A 2020 study found that in the hEDS group, kinesiophobia and BMI together explained 53% of the variance in daily step counts [5]. People who were more fearful of movement simply moved less. This isn’t surprising, but it quantifies just how big an obstacle fear is compared to, say, pain severity alone.
A 2025 study confirmed that kinesiophobia levels were markedly higher in those with hypermobility syndrome compared to healthy controls (TSK scores: 35.34 vs. 20.45, p<0.001), and that kinesiophobia mediated the relationship between proprioceptive deficit and balance impairment [2].
The Fibro Guy has a dedicated, detailed look at what kinesiophobia looks like in hypermobility and EDS and what actually helps, including graded exposure approaches. The short version: you can’t think your way out of kinesiophobia. You have to gradually, safely, accumulate evidence that movement is survivable, and ideally that it makes things better over time.
A multidisciplinary treatment study in hypermobile adolescents combined physical training with exposure in vivo, specifically targeting fear of movement alongside building physical capacity [6]. After treatment, participants showed a 63% reduction in pain intensity, significant reductions in fear (PHODA scores), and improved physical function. This was a small pre-test post-test study (n=14) with no control group, so the findings need replicating in a controlled trial, but the combination of doing and re-learning is consistent with the wider chronic pain literature.
→ Read the full piece on fear of movement in hypermobility and EDS
What Does the Evidence Actually Say About Exercise and Hypermobility?
The honest answer is that the evidence base is growing but still thin. The largest systematic review to date found only 10 eligible studies. That is not the same as saying exercise does not work, it means the research has lagged behind the clinical reality. Here is what we do know, and where the gaps actually sit.
Read MoreThe honest answer is: the evidence base is growing, but it’s still thin compared to other musculoskeletal conditions. A 2022 systematic review by Buryk-Iggers and colleagues, which searched six major databases up to November 2020, identified only 10 eligible studies with a total of 330 participants [7]. Of those, five were RCTs, and only two were rated as high quality with low risk of bias. The review’s conclusion was cautiously positive: “exercise and rehabilitation may be beneficial for various physical and psychological outcomes.”
That’s not exactly a ringing endorsement. But it’s worth understanding why the evidence is limited, rather than taking it to mean exercise doesn’t work. Running high-quality RCTs in hypermobility is genuinely difficult: the population is heterogeneous, diagnosis criteria have changed over time, and getting enough participants for statistical power is hard when you’re excluding people who don’t fit the specific criteria. The lack of evidence is a gap in research funding and design, not a signal that exercise is ineffective.
What We Do Know
A 2024 systematic review on conservative interventions for shoulder symptoms in hEDS/HSD found positive effects from exercise programmes on shoulder function (measured by WOSI), pain, activities of daily living, and both isometric and isokinetic strength [8]. Supervised exercise produced better outcomes than home-based programmes alone.
Neurocognitive rehabilitation, an approach that combines movement with sensory re-education and pain science education, showed significant reductions in pain (p=0.003), fatigue, fear of movement, and disability in people with hEDS and chronic low back pain after three months of treatment. This was a nonrandomised clinical trial (n=18) with no control group, so the effect size needs confirming in a controlled study, but the direction of the result is consistent with the wider motor learning and pain science literature [10].
A 2024 study examining interdisciplinary pain rehabilitation programmes found that people with EDS/HSD benefited from inclusion in these programmes and that their gains were often comparable to those seen in patients with more common chronic pain conditions [11]. This is a meaningful finding: it means that standard rehabilitation infrastructure, when applied thoughtfully, can work for this population.
The GoodHope Exercise and Rehabilitation (GEAR) programme, a structured interdisciplinary programme specifically for EDS and generalised HSD, published its framework in 2021 and described how exercise combined with education and self-management support could address the physical and psychological consequences of connective tissue disorders [12].
The Supervision Question
Across the literature, one finding keeps showing up: supervision matters. The 2021 resistance training RCT by Luder and colleagues found no significant strength improvements from a home-based, self-guided 12-week programme [13]. The doses were likely too low and the heterogeneity too high. Supervised heavy resistance training for women with hypermobility and knee pain, by contrast, proved tolerable and showed positive signals for pain and function [14].
This doesn’t mean you need to be in a clinic for every session. It means the initial framework, the exercise selection, the load progression, the form coaching, needs professional input before going it alone makes sense.
The Principles That Matter

There is no perfect hypermobility exercise. There are principles. Closed chain before open chain. Isometrics before dynamic loading. Proprioception alongside strength. Progress in months not weeks. The biology of connective tissue forces these choices on you whether you like it or not.
Read MoreGiven the specific challenges of hypermobility, there are a handful of principles that shape good exercise programming for this population. These aren’t arbitrary rules. Each one follows from the biology.
Closed-Chain Over Open-Chain (Most of the Time)
Closed-chain exercises, where the foot or hand stays in contact with a surface (squats, press-ups, wall slides), load the joint in a more controlled way than open-chain exercises (leg extensions, bicep curls). In a hypermobile joint, open-chain movements can allow the limb to travel into excessive range without adequate muscular co-contraction to protect the joint. Closed-chain movements naturally encourage co-contraction, which helps protect unstable joints during loading.
This doesn’t mean open-chain exercise is off limits. It means the sequencing matters. Build a foundation of closed-chain control before adding open-chain loading, particularly around the knees, shoulders, and wrists.
Isometrics as a Starting Point
Isometric contractions, where the muscle generates force without joint movement, are a useful entry point for several reasons. They load the tendon and muscle without moving the joint through a range that might be problematic. They also appear to have hypoalgesic effects in many tendinopathy studies, though the evidence is more mixed than the early enthusiasm suggested [15].
For someone with hypermobility who is deconditioned or flare-prone, starting with isometric holds (wall sits, static hand grips, scapular squeezes) allows muscle activation and loading without the risk of joint travel into hypermobile range. When it comes to getting a sensitised system accustomed to exercise again, isometrics are often the most tolerable entry point.
Proprioceptive Training
Given what we know about proprioceptive deficits in hypermobility, targeted proprioceptive training makes logical sense as part of any rehabilitation programme. This includes single-leg balance work, balance board progressions, perturbation training, and exercises that challenge the body to respond to unexpected positional changes.
A 2017 study found that muscle strength is associated with activity limitations in EDS, but that proprioceptive inaccuracy confounds this relationship. The authors concluded that “controlling muscle strength on the basis of proprioceptive input may be more important for reducing activity limitations than just enhancing sheer muscle strength” [16]. Strength training in isolation, without the proprioceptive component, may miss a key piece of the puzzle.
Progressive Overload, Done Carefully
The principle of progressive overload, gradually increasing the challenge placed on the system over time, is as applicable in hypermobility as in any other population. But the gradient of progression needs to be much shallower, and recovery windows much longer, than standard guidelines suggest. Given the evidence that those with hypermobility experience greater DOMS and need more time between sessions [4], a twice-weekly strength programme is often more sustainable than three or four times per week, especially in the early stages.
The target is cumulative loading over months, not weeks. Small increases in resistance, duration, or complexity, consistently applied, will produce meaningful adaptation without triggering the boom-bust cycles that derail so many people’s rehabilitation attempts.
Range of Motion: Neutral, Not Maximum
A key principle when exercising with hypermobility is to train within a controlled range rather than at the extremes of hypermobile range. Loading a knee in full hyperextension, or a shoulder in end-range elevation without scapular control, places force through passive structures that aren’t designed to bear that load. The aim is to build muscular control through the mid-range first, then gradually extend towards full range as that control develops.
→ Read the deeper article on the principles of hypermobility exercise
Muscle Tone: Why You Feel Tight and Weak at the Same Time

Almost everyone with hypermobility describes the same paradox. The muscles feel tight, yet they cannot generate force. Stretch them and the tightness comes back within hours. The reason is muscle tone, the background level of activation your nervous system sets in the muscle, and it is a different thing to muscle length or muscle strength. Once you understand it, a lot of what feels confusing about hypermobile bodies starts to make sense.
Read MoreMuscle tone is the resting electrical activity in your muscles, the background hum that keeps them ready to act. It is not the same as strength, and it is not the same as flexibility. People with hypermobility commonly sit at the low end of the tone spectrum, which produces a recognisable pattern: muscles that feel tight to the touch and on stretch, yet test weak when you actually load them, and that fatigue rapidly during sustained postures.
Why low tone produces a tight feeling
When background tone is low, the muscle has to recruit aggressively to do small tasks. That recruitment is felt as tightness. Stretching the muscle does not address the underlying tone, it just gives temporary relief before the pattern reasserts. The reliable answer is loading. Progressive resistance training, sustained isometric work, and proprioceptive drills all raise tone over time, which is why the same person who stretches every day with no lasting change can feel completely different after eight weeks of strength training.
What to do about it
The practical implication is that exercise prescription for hypermobile bodies should lean heavily on slow, controlled, sustained contractions. Tempo work, paused reps, holds at the hardest position, and isometrics at multiple joint angles all build tone in a way that traditional flexibility work cannot.
Motor Learning: How the Nervous System Builds Reliable Movement

Strengthening a muscle is the easy part. Teaching the nervous system to recruit it reliably, in the right sequence, at the right time, is the work. Motor learning is what turns a movement you can do in front of a mirror into one your body does automatically when you reach for a kettle or step off a kerb. For hypermobile bodies, this layer is often the missing piece between knowing what to do and actually doing it.
Read MoreMotor learning is the process by which the nervous system gets better at producing a movement. It involves the motor cortex, cerebellum, basal ganglia, and the sensory feedback loops that tell the brain whether what happened matched what it intended. For most people, motor learning is invisible. They practice and they improve. In hypermobility, the sensory feedback side of the loop is often unreliable, which slows the whole process down.
Stages of motor learning
There are three classic stages: cognitive, where you have to think hard about every part of the movement, associative, where it starts to feel coordinated but still needs attention, and autonomous, where it runs without conscious effort. Most hypermobile people stall between cognitive and associative because the proprioceptive input that drives consolidation is muddled. The way through is repetition with attention, in environments that give clear feedback, before adding complexity.
Why this matters for rehab
It changes how you design sessions. Short, frequent, attention-rich practice beats long, exhausted sessions where form has degraded. Filming yourself, training in front of a mirror, and using external cues such as a band around the knee to remind it to track outwards, all give the nervous system the feedback it needs to actually learn.
→ Read the full motor learning for hypermobility piece
Want to put motor learning into practice?
The Hypermobility 101 Course walks you through the exact attention-rich movement sessions we use with our clients, so the principles in this section actually translate into your body.
Proprioception and Cortical Maps
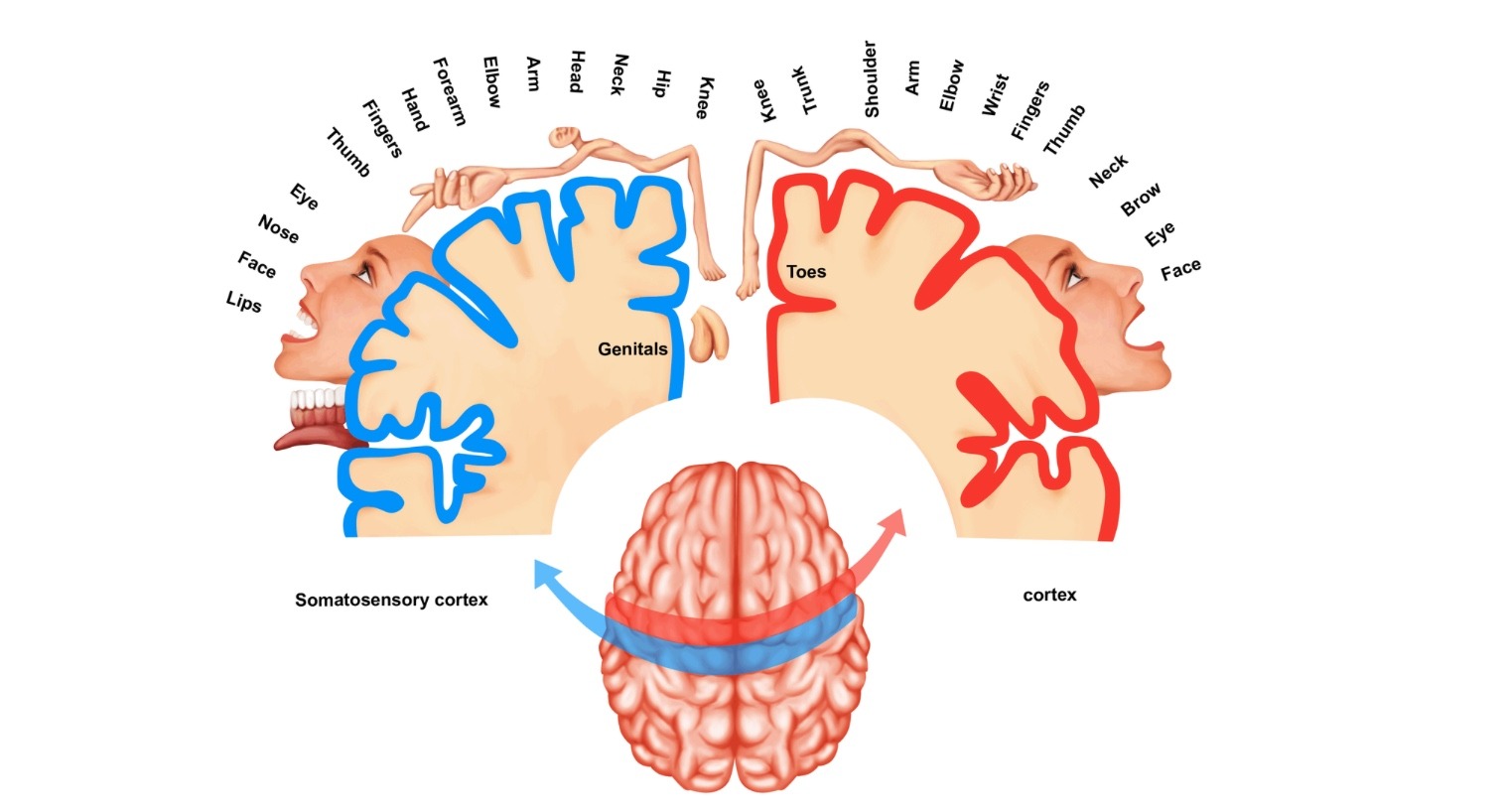
Proprioception is the sense of where your body is without looking. In symptomatic hypermobility it can be unreliable, and the brain that interprets the signal is doing something more sophisticated than the older “fuzzy brain map” story suggested. Train the muscles all you like, if the prediction loop between body and brain is poorly calibrated, the body still feels lost. This is one of the most overlooked pieces of the rehab puzzle, and the evidence around it has moved since 2019.
Read MoreProprioception is built from three things: joint position sense (where a joint is right now), kinaesthesia (how it is moving), and force sense (how much effort is going through it). The signal comes from muscle spindles, Golgi tendon organs, joint capsule receptors, and skin mechanoreceptors, then climbs up to the primary somatosensory cortex where it is laid out on a body map. Crucially, the brain is not passively reading that map. It is predicting where you should be, comparing the prediction to the incoming signal, and adjusting in real time.
Proprioception in hypermobility, what the evidence actually says
The simple version of the story, that hypermobile people automatically have poor proprioception, does not hold up under the recent literature. The more accurate version is this: proprioception is worse in symptomatic hypermobility, but it is not worse just because you are hypermobile. It tends to be worse when there is pain, deconditioning, fatigue, or a history of injury layered on top. People who are hypermobile but asymptomatic often test within typical ranges. That distinction matters, because it changes what you train and why.
The 2019 reframe of the brain map story
For years, chronic pain was explained using a tidy story about cortical reorganisation: pain smudges the body map, and rehab sharpens it back. Under better scanners and more rigorous methods since 2019, the smudging story has been substantially walked back. The brain map is more stable than the older narrative suggested, and pain-related changes are smaller and less reliable than the rehab marketing implies. None of this means sensorimotor training does not help. It does. It just helps for different reasons than the older story claimed.
Why sensorimotor training still works
What proprioceptive and motor learning work actually does is improve the prediction loop. Your brain is constantly forecasting where your body should be and comparing that to incoming signal. When the signal is unreliable, or the prediction is poorly calibrated for your specific joints, the motor system gets fed bad numbers. Slow, precise, attention-rich practice, varied surfaces, tactile cues, and dual-task drills all sharpen that loop. This is why supervised, cue-rich rehab consistently outperforms self-directed wobble board work in the hypermobility literature: the supervisor is constantly correcting the prediction, which is what actually retrains the system.
Zone Moving: The Principle Nobody Mentions

We see lots of things to do with hypermobility rehab on the internet, and time and time again, mechanics, posture, and tissue all get more praise than they warrant. Here is a short video on a basic principle you probably did not realise, and likely no one has ever mentioned to you.

Why Simple Tasks Dislocate Joints
Zone moving is important to ensure that joints are automatically stabilised.
How Dragging Joints Lead To Problems
Excesses in leverage and load make joint stability harder.

Stacking Your Joints Not Working?
You are not alone, there is a reason why it does not work.
For a deeper dive into how the motor system, cortical maps, and proprioception fit together with hypermobility, read our breakdown of Hypermobility and Exercise: Part 1.
Joint-by-Joint: Common Problem Areas

Hypermobility does not affect every joint the same way, and the rehab approach has to reflect that. Knees behave differently to wrists, which behave differently to ribs. This is the headline picture by region, with links into the detailed guides for each area.
Read MoreHypermobility affects joints throughout the entire body, and the rehab approach needs to reflect the different mechanical demands of each region. The sections below link to detailed guides covering each area. This overview gives you the headline picture.
Knees
Knee pain is one of the most common complaints in hypermobility. Recurvatum (hyperextension), patellar instability, and patellofemoral pain are all frequently reported. An RCT in children with JHS found that physiotherapist-prescribed exercise programmes significantly reduced knee pain regardless of whether exercises were performed into the hypermobile range or to neutral [17]. The structured, supervised approach was the key variable. For detailed exercises targeting knee stability in hypermobility, including quadriceps loading strategies and patellar tracking work, there’s a full guide available.
If tibial rotation is a contributing factor, exercises targeting internal tibial rotation and its effects on knee-ankle stability are worth exploring.
Feet and Ankles
Flat arches, ankle instability, and plantar fascia issues are common in this population. The foot is a complex structure that demands proprioceptive control for safe loading during gait and exercise. Specific exercises addressing flat feet and foot arch control in hypermobility are covered in a dedicated guide, including how to build intrinsic foot muscle strength progressively.
Shoulders
Shoulder instability and pain are reported in up to four out of five people with HSD or hEDS [8,9]. The shoulder is inherently the most mobile joint in the body and relies heavily on rotator cuff and scapular stabiliser co-contraction. A systematic review found positive effects from both supervised exercise and kinesiology taping for shoulder symptoms in hEDS/HSD, with exercise producing the most consistent gains in strength and function [8]. Practical guidance on shoulder blade and scapular stabilisation work is available, alongside information on when and how KT tape can support hypermobile joints.
Wrists
Wrist hypermobility affects proprioception, grip strength, and functional capacity. A 2024 study found that chronic wrist hypermobility significantly impairs wrist proprioception, extension strength, grip strength, and function [18]. An RCT comparing wrist stabilisation exercise with orthotic intervention found no significant difference between the two at 12 weeks, suggesting exercise is at least as good as splinting as a conservative management approach [19]. Detailed guidance on managing wrist pain and building wrist stability in hypermobility is covered separately.
Elbows
Elbow hyperextension is a frequent finding on Beighton scoring. When chronic, it can lead to medial instability, lateral epicondylalgia patterns, and ulnar nerve symptoms. Understanding elbow hypermobility and what it means for loading is important before starting upper body resistance training.
Ribs
Rib subluxation and costochondral pain are underappreciated features of hypermobility. They can mimic cardiac symptoms and are often dismissed or misdiagnosed. This is an area where strengthening the thoracic stabilisers matters enormously. A full guide to rib subluxation management in hypermobility is available, along with information on coat hanger pain, a pattern of thoracic and upper cervical pain common in this population.
TMJ (Jaw)
Temporomandibular joint issues are disproportionately common in people with hypermobility. The jaw is subject to the same connective tissue laxity as every other joint, and hypermobile jaw joints can sublux during eating, yawning, and dental procedures. Specific exercises for TMJ pain in hypermobility are covered in a dedicated guide.
Pelvic Floor
The pelvic floor is connective tissue too. Hypermobility can contribute to both hypertonic (over-tight) and hypotonic (weak, lax) pelvic floor dysfunction, and the relationship between them is rarely as straightforward as it appears. A thorough guide to pelvic floor considerations in hypermobility and EDS is available separately.
Scoliosis
Scoliosis has a higher prevalence in people with connective tissue disorders. The interplay between hypermobility and scoliosis shapes what exercises are appropriate and which should be avoided. How scoliosis and hypermobility interact, and how to manage both, is covered in a dedicated post.
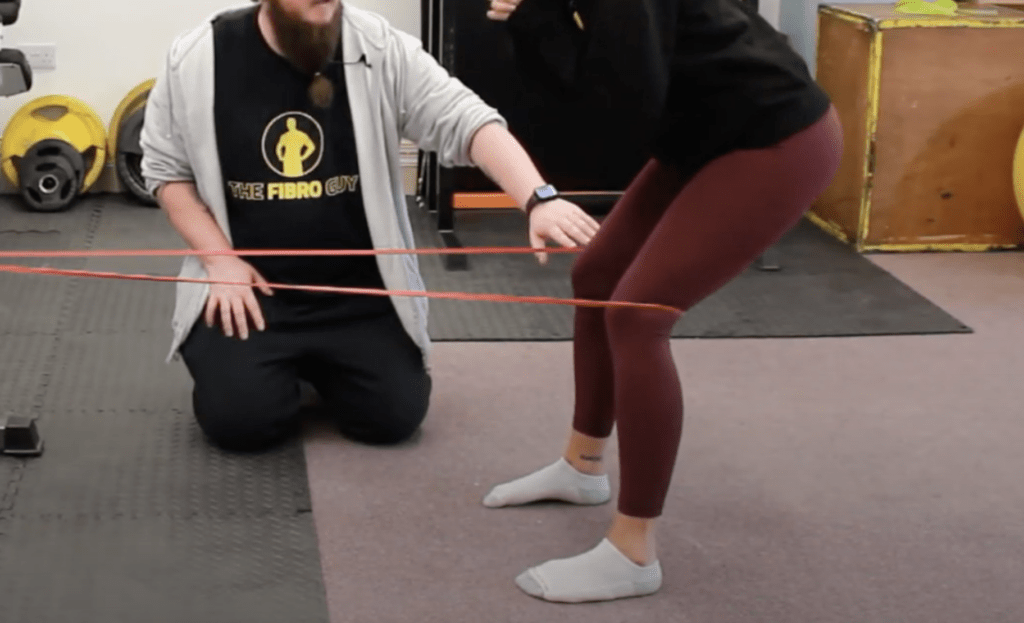
Knee work is the single most asked-about region in our inbox. Here are two of the exercises we use most often with our hypermobile clients, with the full progression in the linked article.
Knee Exercise for Hypermobility
Knee Progression for Hypermobility
Foot Arches: The Foundation Most People Skip
Your foot is not a flat platform that holds you up. It is a dynamic, sensory organ feeding the entire chain above it. If the arches are not doing their job, the knees, hips, and lower back end up compensating, and no amount of glute work will fix it. For hypermobile bodies, the foot is often the missing variable.
Read MoreThe foot is the only part of the body in constant contact with the ground. Every step is a small sensory event, and every sensory event is fed up the chain. When the arches collapse repeatedly, two things happen at once. The mechanical alignment of the knee and hip changes, and the proprioceptive information the brain is getting from the foot becomes unreliable. Both matter, and both are trainable.
Why orthotics are not the whole answer
Orthotics can be a useful short-term tool, particularly during flares or when somebody is dealing with acute pain. As a long-term strategy, they often fail because they replace the muscular work the foot should be doing rather than retraining it. For hypermobile bodies in particular, the foot needs to be trained, not propped.
What foot arch control actually looks like
It is not gripping the floor with your toes. It is the ability to lift the arch under load while keeping the toes long and the heel grounded. The short demonstration in this section shows the basic pattern. Once you can do it standing, the same control needs to transfer into squats, lunges, and eventually into walking and running.
Where this fits in the bigger picture
If your knees collapse inwards, your hip rotators feel constantly tight, or your lower back complains during walking, do not assume the problem is above the foot. Train the arches first, give the brain better information, and see how much of the chain above settles down on its own.
A short demonstration of what foot arch control actually looks like. The full progression sits in the linked article.
Foot Arch Control for Hypermobility
→ Read the full foot arch exercise article for hypermobility
Core Work: Separating Fact from Fiction

Almost every hypermobility programme on the internet leads with planks, bird-dogs, and dead-bugs. The trouble is, traditional core exercises assume a body that braces predictably, and a hypermobile body often does not. Before any specific exercise, it is worth understanding what core stability actually means for a hypermobile system.
Read MoreThe phrase “you just need to strengthen your core” is probably the most common piece of advice those with hypermobility receive, and it’s the most consistently oversimplified. Core stability training is important, but “doing planks” is not the same as building functional spinal stability, and some popular core exercises can actively cause problems for hypermobile spines.
The core isn’t just the rectus abdominis (the six-pack muscles). It includes the deep stabilisers, specifically the transversus abdominis, multifidus, pelvic floor, and diaphragm, which work together to create intra-abdominal pressure and control intersegmental spinal movement. In hypermobility, the global superficial muscles are often overactive and bracing continuously (which is exhausting and doesn’t protect the joints well), while the deep stabilisers aren’t firing with adequate timing or endurance.
A programme that skips past this and loads the spine with high-force exercises early on is likely to cause problems. Core exercise for hypermobility has a full breakdown of where to start, how to progress, and what to avoid. It includes why exercises like traditional sit-ups and certain ab machines are typically counterproductive for this population.
Stretching: What You Need to Know
If you are hypermobile and your muscles feel tight, the answer is rarely more stretching. Tight muscle feel and short muscle length are two different things, and treating one when you have the other usually makes the situation worse, not better.
Read MoreThis section requires a fairly direct statement: most people with hypermobility do not need more flexibility. They already have it in abundance. The common instinct to stretch, which comes from years of cultural messaging about fitness, can actively worsen things in a hypermobile body.
Stretching a joint that already has excessive range doesn’t improve its stability or reduce pain. It may actually increase instability by further loading lax passive structures. Many people with hypermobility report that yoga, when done in a standard way that emphasises range of motion, leads to more pain and more subluxations over time. That’s because joint stability, not joint range, is what’s lacking.
There is a place for gentle movement and mobility work, particularly for managing the muscle guarding and hypertonic patterns that often develop as a secondary response to instability. But this is very different from traditional flexibility stretching. The full guide on the truth about stretching in hypermobility walks through this in detail, including when gentle mobility work is appropriate and when it isn’t.
Pilates and Yoga: What the Evidence Actually Says
Pilates and yoga are the two most commonly recommended movement practices for hypermobility and chronic pain, and the two most commonly oversold. The research base for both has changed in the last few years, and the honest picture is more interesting than the marketing.
Read MoreFor Pilates, the evidence for chronic low back pain has matured: it works as well as other structured exercise, no better, no worse. For hypermobility specifically, until 2026 there was no RCT evidence at all. The first reasonably large trial (an online Pilates programme designed for hypermobility) has now landed, and it shows real but qualified benefits, with caveats around design, attrition, and a structural conflict of interest. For fibromyalgia, the entire global Pilates literature pools to around 265 participants across six trials, anchored on a 2009 pilot, with effects that fade once supervised sessions stop. Pilates also misses two of the most important pieces of hypermobility rehab: motor learning and the difference between active and readiness tone.
For yoga, the picture is similar in shape. There is reasonable evidence for chronic low back pain and for fibromyalgia (where it acts as a general mind-body intervention), but the hypermobility-specific evidence is thin, and standard yoga that emphasises end-range flexibility is a known way for hypermobile joints to get worse. There are forms of yoga that can be safely adapted, but the default class is not one of them.
Our full breakdowns walk through the trials, the methodology, the MCID thresholds, and what each practice actually does and does not do.
→ Read the full Pilates evidence review for hypermobility and fibromyalgia
→ Read the full yoga evidence review for chronic pain and hypermobility
Exercising with POTS

Postural Orthostatic Tachycardia Syndrome runs alongside hypermobility often enough that you cannot design a rehab programme without accounting for it. Standing exercises that look reasonable on paper can trigger pre-syncope. Here is how to structure exercise around an autonomic system that is not playing along.
Read MorePostural Orthostatic Tachycardia Syndrome (POTS) is extremely common in people with hypermobility. Standing up is already a cardiovascular challenge. Add exercise on top of that and you have a complex management problem.
A 2024 scoping review found that while exercise is recommended as a first-line non-pharmacological approach for POTS, the evidence base for people with co-occurring joint hypermobility is thin [20]. The existing evidence from the wider POTS population shows that a structured approach, starting with recumbent/horizontal exercise and gradually progressing towards upright positions over three months, reduces POTS symptoms and improves quality of life.
The key insight from this research is the horizontal-to-upright progression. Starting exercise in a supine or seated position avoids the excessive venous pooling that occurs in upright positions, allows the cardiovascular system to adapt gradually, and prevents the pre-syncopal symptoms that make people give up exercise entirely. Aquatic exercise is particularly well-suited to this population for similar reasons.
There’s a dedicated guide to exercising with POTS that covers the first step that most people miss, along with practical programme suggestions.
Exercise for Children with Hypermobility

Children with hypermobility are not just smaller versions of hypermobile adults. The developing skeleton, motor learning windows, and the influence of fear-avoidance learned early all matter. Done well, structured exercise in childhood can change the trajectory of the condition into adulthood.
Read MoreHypermobility in children presents differently to the adult population in several important ways. Joint laxity is more common in children and typically decreases with age. Hypermobile children are often told their pain is “growing pains” or that they’re being oversensitive, which delays appropriate intervention and can set the scene for kinesiophobia and deconditioning that persists into adulthood.
The evidence in paediatric populations is actually somewhat more encouraging than in adults. A Cochrane-methodology review found strong evidence that enhancing physical fitness is an effective treatment for children with joint hypermobility syndrome, though this was based on a limited number of studies [21].
An RCT in children with JHS and knee pain found that a supervised physiotherapist-prescribed exercise programme significantly reduced knee pain, with a mean 14.5mm reduction on the VAS (p=0.003) [17]. Importantly, the programme worked regardless of whether exercises were performed into the hypermobile range or only to neutral, and no adverse events were reported. The key takeaway: supervised, individualised, progressed exercise is effective and safe for children with hypermobility.
Children also respond strongly to the social and environmental context of exercise. When movement feels safe, supported, and appropriate to their level, they engage with it. When it hurts or they feel judged, avoidance sets in quickly. A full guide to exercise approaches for children with hypermobility covers age-appropriate strategies, school considerations, and how to work with sport and PE teachers.
Running and Higher-Impact Activities
Running gets a bad reputation in the hypermobility world. Some of that is warranted, much of it is not. The question is rarely whether you can run, it is whether your foundation, your tissue capacity, and your loading progression are appropriate to start, and that is a tractable question.
Read MoreRunning is a question that comes up constantly in hypermobility communities. Can I run? Should I run? What happens to my joints when I run?
The honest answer is: it depends, and the same answer applies to most higher-impact activities. Running with hypermobility is possible, but it requires a foundation of joint stability and neuromuscular control that most people haven’t built yet when they start. Going from “barely able to walk without pain” to “5K training plan” is a recipe for injury.
The typical gait problems associated with hypermobility, increased knee valgus, excessive tibial rotation, midfoot collapse, and hip drop, all become more pronounced under the higher forces of running. These are not fixed by running more. They need to be addressed through strength and motor control work first, or they’ll perpetuate the joint loading patterns that cause injury.
That said, when the groundwork is in place, many people with hypermobility run successfully and enjoy it. How to approach running safely with hypermobility covers gait assessment, footwear considerations, load management, and how to build running capacity without repeatedly flaring. For those who prefer lower-impact options, there’s also practical guidance on outdoor exercise that works well alongside hypermobility management.
Pacing: The Missing Piece
Most people with hypermobility are stuck in a boom-bust cycle. Push, crash, recover, push again. Pacing is the dull-sounding skill that breaks the loop, and it is the single biggest determinant of whether an exercise programme actually sticks.
Read MorePacing is probably the most underrated skill in the management of chronic pain and hypermobility. It’s also one of the most misunderstood. It’s not about doing less. It’s about doing consistently, at a level that doesn’t trigger boom-bust cycles.
The pattern most people fall into is familiar: you have a better day, you do more, you pay for it with a flare that sets you back several days. Then you rest until you feel better, have another good day, do too much again, and the cycle repeats. Over months and years, this pattern keeps baseline function low and prevents the gradual adaptation that rehabilitation requires.
Pacing, in a clinical sense, involves establishing a sustainable activity baseline, building from it incrementally regardless of how you feel on any given day, and resisting the pull of both overexertion on good days and excessive rest on bad ones. It’s one of the most evidence-supported approaches for chronic musculoskeletal conditions and chronic pain [22].
The full evidence-based guide to pacing strategies for EDS and chronic pain covers the theory, the practical implementation, and how to adapt pacing as you build capacity.
Pacing also applies specifically to those getting started with exercise when hypermobility makes movement difficult. The early stages are about building the habit and the recovery capacity, not hitting targets.
Sleep and Hypermobility

Sleep is where adaptation actually happens. Without it, the loading you do in the gym does not consolidate, pain processing dysregulates, and autonomic symptoms get worse. For people with hypermobility, sleep architecture itself is often disrupted, and that needs handling alongside any exercise plan.
Read MoreTackling hypermobility challenges does not end when the sun goes down. In fact, that is when a fresh journey begins. Our article, Sleep and Hypermobility, sheds light on why sleep is vital, the distinct sleep complications for those with hypermobility and EDS, and tailored strategies to better your sleep routine.
Explore sleep positions, how to set up a conducive sleep environment, and understand how sleep deprivation amplifies pain. The full guide covers actionable steps aimed at enhancing your sleep quality alongside hypermobility.
Hypermobility and Nutrition

Nutrition will not fix hypermobility, but it changes the system you are loading. Energy availability, protein intake, and dietary patterns all affect recovery, tissue tolerance, and how you feel between sessions. Here is what the evidence actually supports, and what gets oversold.
Read MoreWhether you are new to the EDS community, a long-time warrior, or a loved one seeking to understand and support, hypermobility and Ehlers-Danlos syndrome diets matter more than most people realise.
We explore the role of nutrition in EDS and hypermobility management, address common nutritional deficiencies, and provide practical diet recommendations and strategies. To help on this mammoth task, dietician Katie Mednik shared her expertise and fact-checked the article.
Supplements That Support Exercise
The hypermobility supplement market is loud. Collagen, magnesium, vitamin C, the list goes on. Some of these have a defensible role alongside training, most are oversold. Here is what to actually pay attention to, and what to leave alone.
Read MoreThe supplement industry loves chronic pain populations, and most of what’s marketed at people with hypermobility is either unproven or useless. One exception is worth covering here: creatine.
Creatine monohydrate is the most well-researched performance supplement in existence. Its primary mechanisms are relevant to the challenges of hypermobility: it increases phosphocreatine stores, improving energy availability for high-intensity muscle contractions; it supports lean mass development; and emerging research suggests potential roles in reducing muscle damage markers and improving recovery from exercise.
For someone working to build the muscular support their joints need, having adequate creatine available in the muscle can make a meaningful difference to training quality and recovery. A full breakdown of creatine’s benefits for hypermobility and EDS is available, including dosing guidance and what the evidence actually shows for this population specifically.
Beyond creatine, the basics matter: adequate protein intake to support muscle repair and growth, vitamin D if deficient (common in those who spend significant time indoors due to symptoms), and magnesium for muscle function. None of these replace exercise, but they can support the recovery and adaptation that makes exercise productive.
→ Read the full article on creatine for hypermobility and EDS
KT Taping for Hypermobility

Taping is not magic, and it is not nothing. Used well, kinesiology tape can give a hypermobile joint enough proprioceptive feedback to load more confidently during a session. Used as a substitute for building muscular control, it never delivers what it promises. Here is when and how to use it.
Read MoreKT tape is one of the most asked-about tools in hypermobility. It is not a magic fix, but applied correctly it can provide a useful sensory cue while you rebuild stability through training. Our full article on KT tape walks through the evidence, when it helps, when it does not, and how to apply it for the most common hypermobile joints.
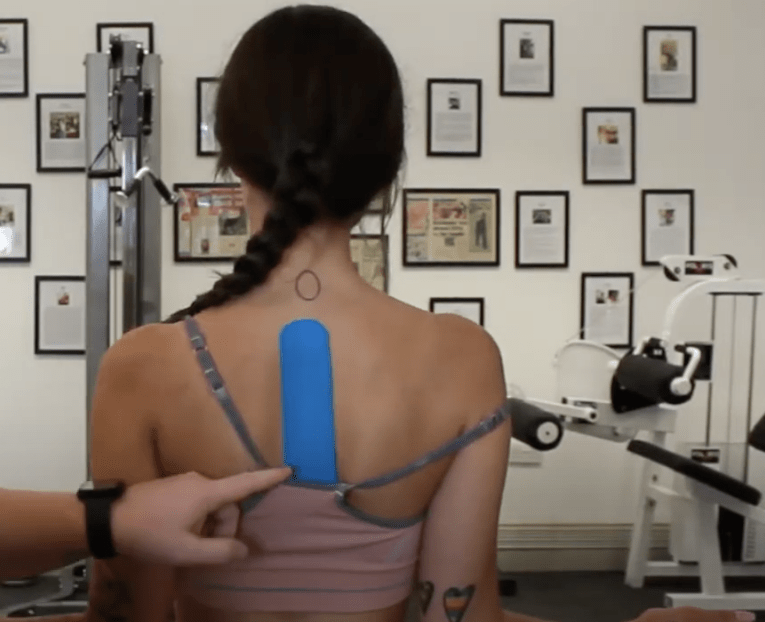
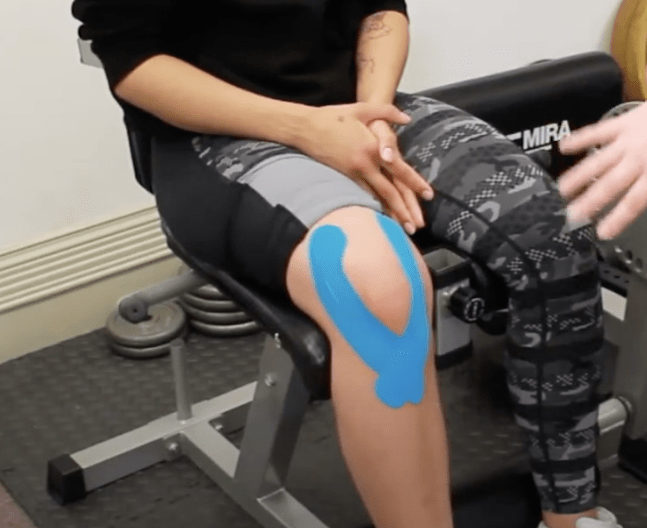

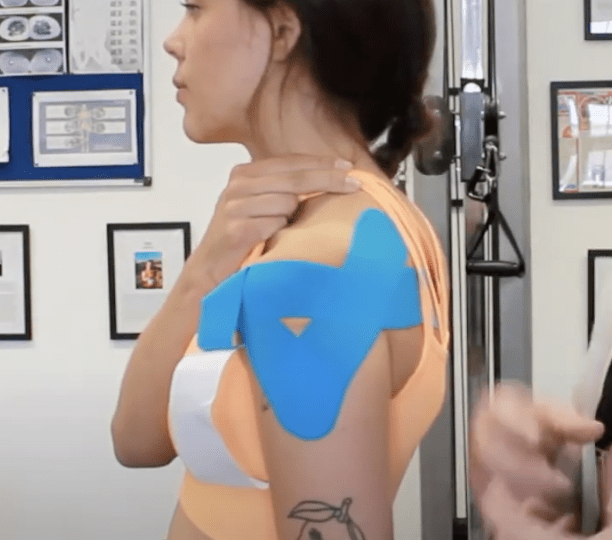

Two short demonstrations from our taping guide, showing the patterns we use most often. The full set, including taping for specific joints, sits in the dedicated article.
KT Taping for Hypermobility, Part One
KT Taping for Hypermobility, Part Two
→ Read the full KT tape for hypermobility and EDS article

Want the full taping system?
The KT Taping Course walks you through every taping pattern we use, joint by joint, with the reasoning behind each one. Built for hypermobile bodies, not generic sports taping.
Braces, Supports and the Body Braid
Tape is not the only external aid people ask about. Braces, compression garments, and the Body Braid all get marketed to hypermobile bodies on the promise of better posture and stability. Some of that holds up, a lot of it does not. Here is how to think about supports without wasting your money.
Read MoreThe Body Braid is the one that comes up most. It is a spiral elastic garment that wraps the torso and limbs in a figure of eight, and it is marketed hard on posture, balance, and proprioception, with a 2025 study often held up as proof. Having read that study and the papers it leans on in full, the honest position is that the strongest marketing claims run well ahead of the data, even though the garment itself is well made and some people find it genuinely useful to wear.
The principle is the same one that governs tape and bracing generally. A support can give the nervous system a helpful sensory cue in the short term, but it works best as a temporary prompt while you build real muscular control, not as a replacement for it. If a garment helps you move more confidently while you train, that is a reasonable use. Expecting it to hold a body together on its own is where the money tends to get wasted.
Putting It Together: Where to Start
If you have read this far, the principles will feel like a lot. They are. But sequencing them is straightforward, and most people start in roughly the same place. Here is the entry point, the first three to four weeks, and what to track so you know whether things are going the right way.
Read MoreGiven everything above, what does a sensible starting point actually look like? A few practical principles:
Start lower than you think you need to. If you’re deconditioned or in a high-pain period, the first goal is to establish a consistent, non-aggravating movement habit. Even five minutes of gentle closed-chain exercises twice a day is a foundation. You can build from there.
Address the basics first. Foot and ankle control, scapular stability, hip control, and basic trunk co-contraction are the building blocks. Loading compound movements on top of unstable foundations will create problems.
Get professional input if possible. The supervised exercise research consistently outperforms the self-directed research. A physiotherapist or rehabilitation specialist with genuine experience in hypermobility can save months of trial and error.
Don’t skip pacing. A brilliant exercise programme that triggers repeated flares will be abandoned. A modest programme that you can sustain for 12 months will produce far better outcomes than an ambitious one you do for three weeks.
For those who’ve struggled with exercise previously and want to practical, specific exercise tips for hypermobility, there’s a guide covering the most common mistakes and how to avoid them. And for those managing hypermobility alongside fibromyalgia, the guide on exercise when you also have fibromyalgia addresses the overlapping challenges of both conditions.
Chronic Pain, Relationships and Intimacy

The bit of chronic pain that gets skipped in clinic is the bit that affects your relationship, your sex life, and how you talk about any of it with the person you share a bed with. Sleep gets asked about. Walking the dog gets asked about. The fact your hip subluxes when you change position, or that you crash for three days after anything more than a cuddle, somehow does not.
That gap is where most of the hidden suffering sits, and it shows up across hypermobility, fibromyalgia, POTS and ME/CFS. We have a full guide covering disclosure to new partners, communication inside long term relationships, positioning, pacing intimacy, the LGBTQ and polyamorous experience of chronic pain, and how to look after a body that does not always cooperate.
→ Read the full guide: Chronic Pain, Relationships and Intimacy
Where to Go From Here
This guide is the educational foundation. If you want to take the same frameworks deeper, with live Q&A, exercise demonstrations, and the chance to ask us anything about your own situation, the Hypermobility Live Workshop is the next step.
Read MoreReading about exercise is the easy bit. Actually doing it safely, with the right progressions, in a body that doesn’t behave the way the textbooks say it should, that’s where it gets interesting.
The Hypermobility Live Workshop is where we go through all of this properly. Four weeks, live sessions, and you can ask us about your specific joints, your specific flare patterns, whatever you need. It’s basically what we do in our studios, but online. Or if you want something self-paced, the course library has you covered.

Ready to work through this with structure and support?
This guide is the educational foundation. The Hypermobility Live Workshop takes the same frameworks deeper, with live Q&A sessions where you can ask us anything and apply what you have learned to your own body. Two free courses are included.
References
- Long M, Kiru L, Kassam J, Strutton PH, Alexander CM. An investigation of the control of quadriceps in people who are hypermobile; a case control design. Do the results impact our choice of exercise for people with symptomatic hypermobility? BMC Musculoskelet Disord. 2022;23:607. doi: 10.1186/s12891-022-05540-1
- ALMohiza MA, Reddy RS. Exploring the dynamics of stability and lumbar proprioception in hypermobility syndrome: a comparative and mediation analysis. J Orthop Surg Res. 2025;20:285. doi: 10.1186/s13018-025-05683-6
- Schubert-Hjalmarsson E, Fasth A, Ickmans K, Söderpalm AC, Lundberg M. Exploring signs of central sensitization in adolescents with hypermobility spectrum disorder or hypermobile Ehlers-Danlos syndrome. Eur J Pain. 2024;29(1):e4754. doi: 10.1002/ejp.4754
- Ostuni NF, Marinello CA, Luzhnyy T, Pawlikowski A, Vlasaty C, Thomatos G, Douris PC. The effect of joint hypermobility syndrome on DOMS and recovery time. Int J Sports Phys Ther. 2024;19(2). doi: 10.26603/001c.91644
- Coussens M, De Wandele I, Pacey V, Malfait F, De Craemer M, Demeyer H, Rombaut L, Calders P. Physical activity and sleep in patients with hypermobile Ehlers-Danlos syndrome and patients with generalized hypermobility spectrum disorder. Edorium J Disabil Rehabil. 2020. doi: 10.5348/100049d05mc2020ra
- Van Meulenbroek T, Conijn AEA, Huijnen IPJ, Engelbert RHH, Verbunt JA. Multidisciplinary treatment for hypermobile adolescents with chronic musculoskeletal pain. J Rehabil Med Clin Commun. 2020;3:1000033. doi: 10.2340/20030711-1000033
- Buryk-Iggers S, Mittal N, Santa Mina D, Adams SC, Englesakis M, Rachinsky M, et al. Exercise and rehabilitation in people with Ehlers-Danlos syndrome: a systematic review. Arch Rehabil Res Clin Transl. 2022;4(2):100189. doi: 10.1016/j.arrct.2022.100189
- Higo A, Palmer S, Liaghat B, Tallis J, Silvester L, Pearce G. The effectiveness of conservative interventions on pain, function, and quality of life in adults with hypermobile Ehlers-Danlos syndrome/hypermobility spectrum disorders and shoulder symptoms: a systematic review. Arch Rehabil Res Clin Transl. 2024;6(3):100360. doi: 10.1016/j.arrct.2024.100360
- Liaghat B, Skou ST, Søndergaard J, Boyle E, Søgaard K, Juul-Christensen B. A randomised controlled trial of heavy shoulder strengthening exercise in patients with hypermobility spectrum disorder or hypermobile Ehlers-Danlos syndrome and long-lasting shoulder complaints: study protocol for the Shoulder-MOBILEX study. Trials. 2020;21(1):992. doi: 10.1186/s13063-020-04892-0
- Celletti C, Paolucci T, Maggi L, Volpi G, Billi M, Mollica R, Camerota F. Pain management through neurocognitive therapeutic exercises in hypermobile Ehlers-Danlos syndrome patients with chronic low back pain. Biomed Res Int. 2021;2021:6664864. doi: 10.1155/2021/6664864
- Molander P, Novo M, Ringqvist Å, Hållstam A, Hesser H, Löfgren M, Stålnacke BM, Gerdle B. Interdisciplinary pain rehabilitation for patients with Ehlers-Danlos syndrome and hypermobility spectrum disorders. J Rehabil Med. 2024;56:jrm12431. doi: 10.2340/jrm.v56.12431
- Mittal N, Santa Mina D, Buryk-Iggers S, et al. The GoodHope Exercise and Rehabilitation (GEAR) program for people with Ehlers-Danlos syndromes and generalized hypermobility spectrum disorders. Front Rehabil Sci. 2021;2:769792. doi: 10.3389/fresc.2021.769792
- Luder G, Aeberli D, Mebes CM, Haupt-Bertschy B, Baeyens JP, Verra ML. Effect of resistance training on muscle properties and function in women with generalized joint hypermobility: a single-blind pragmatic randomized controlled trial. BMC Sports Sci Med Rehabil. 2021;13:10. doi: 10.1186/s13102-021-00238-8
- Henriksen P, Junge T, Bojsen-Møller J, Juul-Kristensen B, Thorlund JB. Supervised, heavy resistance training is tolerated and potentially beneficial in women with knee pain and knee joint hypermobility: a case series. Pain Res Manag. 2022;2022:8367134. doi: 10.1155/2022/8367134
- Clifford C, Challoumas D, Paul L, Syme G, Millar N. Effectiveness of isometric exercise in the management of tendinopathy: a systematic review and meta-analysis of randomised trials. BMJ Open Sport Exerc Med. 2020;6(1):e000760. doi: 10.1136/bmjsem-2020-000760
- Scheper M, Rombaut L, de Vries J, De Wandele I, van der Esch M, Visser B, Malfait F, Calders P, Engelbert R. The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception. Disabil Rehabil. 2017;39(14):1391-1397. doi: 10.1080/09638288.2016.1196396
- Pacey V, Tofts L, Adams R, Munns C, Nicholson L. Exercise in children with joint hypermobility syndrome and knee pain: a randomised controlled trial comparing exercise into hypermobile versus neutral knee extension. Pediatr Rheumatol Online J. 2013;11:30. doi: 10.1186/1546-0096-11-30
- Karagiannopoulos C, Griech S. Impact of chronic wrist hypermobility on proprioception, strength, and functional performance in young adults. J Hand Ther. 2024;37(2):209-217. doi: 10.1016/j.jht.2023.10.001
- Lindholm S, Claesson L. Wrist stabilising exercise versus hand orthotic intervention for persons with hypermobility: a randomised clinical trial. Clin Rehabil. 2025. doi: 10.1177/02692155241293265
- Peebles KC, Jacobs C, Makaroff L, Pacey V. The use and effectiveness of exercise for managing postural orthostatic tachycardia syndrome in young adults with joint hypermobility and related conditions: a scoping review. Auton Neurosci. 2024;252:103156. doi: 10.1016/j.autneu.2024.103156
- Scheper MC, Engelbert RHH, Rameckers EAA, Verbunt J, Remvig L, Juul-Kristensen B. Children with generalised joint hypermobility and musculoskeletal complaints: state of the art on diagnostics, clinical characteristics, and treatment. Biomed Res Int. 2013;2013:121054. doi: 10.1155/2013/121054
- Andrews NE, Strong J, Meredith PJ. Activity pacing, avoidance, endurance, and associations with patient functioning in chronic pain: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2012;93(11):2109-2121. doi: 10.1016/j.apmr.2012.05.029
Additional references: Muscle Tone
Sourced from Muscle Tone. These references support the deeper discussion in the linked blog.
- Greenwood NL, Duffell LD, Alexander CM, McGregor AH. (2011) Electromyographic activity of pelvic and lower limb muscles during postural tasks in people with benign joint hypermobility syndrome and non hypermobile people. A pilot study. Manual Therapy 16(6):623-628. doi: 10.1016/j.math.2011.07.005
- Junge T, Wedderkopp N, Thorlund JB, Søgaard K, Juul-Kristensen B. (2015) Altered knee joint neuromuscular control during landing from a jump in 10-15 year old children with Generalised Joint Hypermobility. A substudy of the CHAMPS-study Denmark. Journal of Electromyography and Kinesiology 25(3):501-507. doi: 10.1016/j.jelekin.2015.02.011
- Rombaut L, Malfait F, De Wandele I, Taes Y, Thijs Y, De Paepe A, Calders P. (2012) Muscle mass, muscle strength, functional performance, and physical impairment in women with the hypermobility type of Ehlers-Danlos syndrome. Arthritis Care & Research 64(10):1584-1592. doi: 10.1002/acr.21726
- Coussens M, Calders P, Lapauw B, Celie B, Banica T, De Wandele I, Pacey V, Malfait F, Rombaut L. (2021) Does Muscle Strength Change Over Time in Patients With Hypermobile Ehlers-Danlos Syndrome/Hypermobility Spectrum Disorder? An Eight-Year Follow-Up Study. Arthritis Care & Research 73(7):1041-1048. doi: 10.1002/acr.24220
- Scheper M, Rombaut L, de Vries J, De Wandele I, van der Esch M, Visser B, Malfait F, Calders P, Engelbert R. (2017) The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception. Disability and Rehabilitation 39(14):1391-1397. doi: 10.1080/09638288.2016.1196396
- Winter L, Huang Q, Sertic JVL, Konczak J. (2022) The Effectiveness of Proprioceptive Training for Improving Motor Performance and Motor Dysfunction: A Systematic Review. Frontiers in Rehabilitation Sciences 3:830166. doi: 10.3389/fresc.2022.830166
- Moutzouri M, Coutts F, Gliatis J, Billis E, Tsepis E, Gleeson N. (2019) Early initiation of home-based sensori-motor training improves muscle strength, activation and size in patients after knee replacement: a secondary analysis of a controlled clinical trial. BMC Musculoskeletal Disorders 20(1):231. doi: 10.1186/s12891-019-2575-3
- Celletti C, Paolucci T, Maggi L, Volpi G, Billi M, Mollica R, Camerota F. (2021) Pain Management through Neurocognitive Therapeutic Exercises in Hypermobile Ehlers-Danlos Syndrome Patients with Chronic Low Back Pain. BioMed Research International 2021:6664864. doi: 10.1155/2021/6664864
- van Meulenbroek T, Conijn AEA, Huijnen IPJ, Engelbert RHH, Verbunt JA. (2020) Multidisciplinary Treatment for Hypermobile Adolescents with Chronic Musculoskeletal Pain. Journal of Rehabilitation Medicine, Clinical Communications 3:1000033. doi: 10.2340/20030711-1000033
Additional references: Motor Learning
Sourced from Motor Learning. These references support the deeper discussion in the linked blog.
- Scheper M, Rombaut L, de Vries J, De Wandele I, van der Esch M, Visser B, Malfait F, Calders P, Engelbert R. (2017) The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception. Disability and Rehabilitation 39(14):1391-1397. doi: 10.1080/09638288.2016.1196396
- Wulf G, Lewthwaite R. (2016) Optimizing performance through intrinsic motivation and attention for learning: The OPTIMAL theory of motor learning. Psychonomic Bulletin & Review 23(5):1382-1414. doi: 10.3758/s13423-015-0999-9
- Chua LK, Jimenez-Diaz J, Lewthwaite R, Kim T, Wulf G. (2021) Superiority of external attentional focus for motor performance and learning: Systematic reviews and meta-analyses. Psychological Bulletin 147(6):618-645. doi: 10.1037/bul0000335
- McKay B, Bacelar MFB, Parma JO, Miller MW, Carter MJ. (2025) The combination of reporting bias and underpowered study designs has substantially exaggerated the motor learning benefits of self-controlled practice and enhanced expectancies: a meta-analysis. International Review of Sport and Exercise Psychology 18(1):242-262. doi: 10.1080/1750984X.2023.2207255
- Moseley GL. (2004) Graded motor imagery is effective for long-standing complex regional pain syndrome: a randomised controlled trial. Pain 108(1-2):192-198. doi: 10.1016/j.pain.2004.01.006
- Sale DG. (1988) Neural adaptation to resistance training. Medicine & Science in Sports & Exercise 20(5 Suppl):S135-S145. doi: 10.1249/00005768-198810001-00009
- Folland JP, Williams AG. (2007) The adaptations to strength training: morphological and neurological contributions to increased strength. Sports Medicine 37(2):145-168. doi: 10.2165/00007256-200737020-00004
- Rice DA, McNair PJ. (2010) Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Seminars in Arthritis and Rheumatism 40(3):250-266. doi: 10.1016/j.semarthrit.2009.10.001
- Tsao H, Galea MP, Hodges PW. (2008) Reorganization of the motor cortex is associated with postural control deficits in recurrent low back pain. Brain 131(8):2161-2171. doi: 10.1093/brain/awn154
- Tsao H, Danneels LA, Hodges PW. (2011) ISSLS prize winner: Smudging the motor brain in young adults with recurrent low back pain. Spine 36(21):1721-1727. doi: 10.1097/BRS.0b013e31821c4267
- Dantzer R, Kelley KW. (2007) Twenty years of research on cytokine-induced sickness behavior. Brain, Behavior, and Immunity 21(2):153-160. doi: 10.1016/j.bbi.2006.09.006
Additional references: Cortical Maps and Proprioception
Sourced from Cortical Maps and Proprioception. These references support the deeper discussion in the linked blog.
- Rombaut L, De Paepe A, Malfait F, Cools A, Calders P. Joint position sense and vibratory perception sense in patients with Ehlers-Danlos syndrome type III (hypermobility type). Clin Rheumatol. 2010;29(3):289 to 295. doi:10.1007/s10067-009-1320-y
- Hall MG, Ferrell WR, Sturrock RD, Hamblen DL, Baxendale RH. The effect of the hypermobility syndrome on knee joint proprioception. Br J Rheumatol. 1995;34(2):121 to 125. doi:10.1093/rheumatology/34.2.121
- Fatoye F, Palmer S, Macmillan F, Rowe P, van der Linden M. Proprioception and muscle torque deficits in children with hypermobility syndrome. Rheumatology (Oxford). 2009;48(2):152 to 157. doi:10.1093/rheumatology/ken435
- Mallik AK, Ferrell WR, McDonald AG, Sturrock RD. Impaired proprioceptive acuity at the proximal interphalangeal joint in patients with the hypermobility syndrome. Br J Rheumatol. 1994;33(7):631 to 637. doi:10.1093/rheumatology/33.7.631
- Akaras E, Deniz G, Eymir M, Sönmez M. The effects of joint hypermobility on strength, proprioception and functional performance. Sci Rep. 2025;15. doi:10.1038/s41598-025-24199-x
- Ituen OA, Smits-Engelsman B, Ferguson G, Duysens J. Proprioception and its relationship with range of motion in hypermobile and normal mobile children. Exp Brain Res. 2024;242(12):2833 to 2845. doi:10.1007/s00221-024-06937-1
- Ituen OA, Ferguson G, Duysens J, Smits-Engelsman B. The strength of balance: strength and dynamic balance in children with and without hypermobility. PLoS ONE. 2024;19(6):e0302218. doi:10.1371/journal.pone.0302218
- Scheper MC, Rombaut L, de Vries J, de Wandele I, van der Esch M, Visser B, Malfait F, Calders P, Engelbert R. The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception. Disabil Rehabil. 2017;39(14):1391 to 1397. doi:10.1080/09638288.2016.1196396
- Scheper MC, de Vries JE, Verbunt J, Engelbert RH. Chronic pain in hypermobility syndrome and Ehlers-Danlos syndrome (hypermobility type): it is a challenge. J Pain Res. 2015;8:591 to 601. doi:10.2147/JPR.S64251
- Rombaut L, Malfait F, De Wandele I, Thijs Y, Palmans T, De Paepe A, Calders P. Balance, gait, falls and fear of falling in women with the hypermobility type of Ehlers-Danlos syndrome. Arthritis Care Res. 2011;63(10):1432 to 1439. doi:10.1002/acr.20557
- Dupuy EG, Leconte P, Vlamynck E, Sultan A, Chesneau C, Denise P, Besnard S, Bienvenu B, Decker LM. Ehlers-Danlos syndrome, hypermobility type: impact of somatosensory orthoses on postural control (a pilot study). Front Hum Neurosci. 2017;11:283. doi:10.3389/fnhum.2017.00283
- Long M, Kiru L, Kassam J, Strutton PH, Alexander CM. An investigation of the control of quadriceps in people who are hypermobile: a case control design. BMC Musculoskelet Disord. 2022;23:530. doi:10.1186/s12891-022-05540-1
- Clayton HA, Jones SAH, Henriques DYP. Proprioceptive precision is impaired in Ehlers-Danlos syndrome. SpringerPlus. 2015;4:323. doi:10.1186/s40064-015-1089-1
- ALMohiza MA, Reddy RS. Exploring the dynamics of stability and lumbar proprioception in hypermobility syndrome: a comparative and mediation analysis. J Orthop Surg Res. 2025;20:282. doi:10.1186/s13018-025-05683-6
- Whitmore M, Barker B, Chudej K, Goines C, Kester J, Campbell H, Jeffcoat A, Castleberry B, Lowder TW. A novel method of assessing balance and postural sway in patients with hypermobile Ehlers-Danlos syndrome. Front Med. 2023;10:1135473. doi:10.3389/fmed.2023.1135473
- Mancini F, Wang AP, Schira MM, Isherwood ZJ, McAuley JH, Iannetti GD, Sereno MI, Moseley GL, Rae CD. Fine-grained mapping of cortical somatotopies in chronic complex regional pain syndrome. J Neurosci. 2019;39(46):9185 to 9196. doi:10.1523/JNEUROSCI.2005-18.2019
- Makin TR, Scholz J, Filippini N, Henderson Slater D, Tracey I, Johansen-Berg H. Phantom pain is associated with preserved structure and function in the former hand area. Nat Commun. 2013;4:1570. doi:10.1038/ncomms2571
- Makin TR, Bensmaia SJ. Stability of sensory topographies in adult cortex. Trends Cogn Sci. 2017;21(3):195 to 204. doi:10.1016/j.tics.2017.01.002
- Flor H, Elbert T, Knecht S, Wienbruch C, Pantev C, Birbaumer N, Larbig W, Taub E. Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature. 1995;375(6531):482 to 484. doi:10.1038/375482a0
- Moseley GL, Gallace A, Spence C. Bodily illusions in health and disease: physiological and clinical perspectives and the concept of a cortical “body matrix”. Neurosci Biobehav Rev. 2012;36(1):34 to 46. doi:10.1016/j.neubiorev.2011.03.013
- Moseley GL, Flor H. Targeting cortical representations in the treatment of chronic pain: a review. Neurorehabil Neural Repair. 2012;26(6):646 to 652. doi:10.1177/1545968311433209
- Schabrun SM, Elgueta-Cancino EL, Hodges PW. Smudging of the motor cortex is related to the severity of low back pain. Spine. 2017;42(15):1172 to 1178. doi:10.1097/BRS.0000000000000938
- Catley MJ, O’Connell NE, Berryman C, Ayhan FF, Moseley GL. Is tactile acuity altered in people with chronic pain? A systematic review and meta-analysis. J Pain. 2014;15(10):985 to 1000. doi:10.1016/j.jpain.2014.06.009
- Hotta J, Harno H, Saari J, Forss N, Hari R. Somatotopic disruption of the functional connectivity of the primary sensorimotor cortex in complex regional pain syndrome type 1. Hum Brain Mapp. 2023;44(15):e26513. doi:10.1002/hbm.26513
- Makin TR, Scholz J, Henderson Slater D, Johansen-Berg H, Tracey I. Reassessing cortical reorganization in the primary sensorimotor cortex following arm amputation. Brain. 2015;138(8):2172 to 2177. doi:10.1093/brain/awv161
- Kikkert S, Johansen-Berg H, Tracey I, Makin TR. Reaffirming the link between chronic phantom limb pain and maintained missing hand representation. Cortex. 2018;106:174 to 184. doi:10.1016/j.cortex.2018.05.013
- Schone HR, Maimon-Mor RO, Kollamkulam M, Szymanska M, Gerrand C, Woollard A, Kang NV, Baker CI, Makin TR. Stable cortical body maps before and after arm amputation. Nat Neurosci. 2025;28:1678 to 1687. doi:10.1038/s41593-025-02037-7
- Makin TR, Flor H. Brain (re)organisation following amputation: implications for phantom limb pain. NeuroImage. 2020;218:116943. doi:10.1016/j.neuroimage.2020.116943
- Hanzlíková I, Ruská A, Hébert-Losier K, Jančíková K. No significant links between somatognosia, stereognosia and hypermobility: sensory processing unlikely to drive common complaints in hypermobile population. BMC Musculoskelet Disord. 2025;26:08307. doi:10.1186/s12891-025-08307-6
- Mancini F, Bauleo A, Cole J, Lui F, Porro CA, Haggard P, Iannetti GD. Whole-body mapping of spatial acuity for pain and touch. Ann Neurol. 2014;75(6):917 to 924. doi:10.1002/ana.24179
- Bagg MK, Wand BM, Cashin AG, Lee H, Hübscher M, Stanton TR, O’Connell NE, O’Hagan ET, Rizzo RRN, Wewege MA, Rabey M, Goodall S, Saing S, Lo SN, Luomajoki H, Herbert RD, Maher CG, Moseley GL, McAuley JH. Effect of graded sensorimotor retraining on pain intensity in patients with chronic low back pain: a randomized clinical trial. JAMA. 2022;328(5):430 to 439. doi:10.1001/jama.2022.9930
- Cashin AG, Lee H, Wand BM, Bagg MK, O’Hagan ET, Rizzo RRN, Stanton TR, Moseley GL, McAuley JH. Mechanisms of education and graded sensorimotor retraining in people with chronic low back pain: a mediation analysis. Pain. 2023;164(6):1202 to 1213. doi:10.1097/j.pain.0000000000002978
- Malfliet A, Kregel J, Coppieters I, De Pauw R, Meeus M, Roussel N, Cagnie B, Danneels L, Nijs J. Effect of pain neuroscience education combined with cognition-targeted motor control training on chronic spinal pain: a randomized clinical trial. JAMA Neurol. 2018;75(7):808 to 817. doi:10.1001/jamaneurol.2018.0492
- Donati D, Giorgi F, Platano D, Tedeschi R, Boccolari P, Berti L. Breaking the cycle of pain: the role of graded motor imagery and mirror therapy in complex regional pain syndrome. Biomedicines. 2024;12(9):2140. doi:10.3390/biomedicines12092140
- Krakauer JW, Hadjiosif AM, Xu J, Wong AL, Haith AM. Motor learning. Compr Physiol. 2019;9(2):613 to 663. doi:10.1002/cphy.c170043
- Wulf G, Lewthwaite R. Optimizing performance through intrinsic motivation and attention for learning: the OPTIMAL theory of motor learning. Psychon Bull Rev. 2016;23(5):1382 to 1414. doi:10.3758/s13423-015-0999-9
- Chua L-K, Jiménez-Díaz J, Lewthwaite R, Kim T, Wulf G. Superiority of external attentional focus for motor performance and learning: systematic reviews and meta-analyses. Psychol Bull. 2021;147(6):618 to 645. doi:10.1037/bul0000335
- Seo HG, Yun SJ, Farrens A, Johnson C, Reinkensmeyer DJ. A systematic review of the learning dynamics of proprioception training: specificity, acquisition, retention and transfer. Neurorehabil Neural Repair. 2023;37(10):697 to 713. doi:10.1177/15459683231207354
- Sienko KH, Balkwill MD, Oddsson LIE, Wall C. The effect of vibrotactile feedback on postural sway during locomotor activities. J Neuroeng Rehabil. 2013;10:93. doi:10.1186/1743-0003-10-93
- Anctil N, Malenfant Z, Cyr J-P, Turcot K, Simoneau M. Less vibrotactile feedback is effective to improve human balance control during sensory cues alteration. Sensors. 2022;22(17):6432. doi:10.3390/s22176432
- de Vasconcelos GS, Cini A, Sbruzzi G, Lima CS. Effects of proprioceptive training on the incidence of ankle sprain in athletes: systematic review and meta-analysis. Clin Rehabil. 2018;32(12):1581 to 1590. doi:10.1177/0269215518788683
- Chiaramonte R, Bonfiglio M, Leonforte P, Coltraro GL, Guerrera CS, Vecchio M. Proprioceptive and dual-task training: the key of stroke rehabilitation, a systematic review. J Funct Morphol Kinesiol. 2022;7(3):53. doi:10.3390/jfmk7030053
- Higo A, Palmer S, Liaghat B, Tallis J, Silvester L, Pearce G. The effectiveness of conservative interventions on pain, function and quality of life in adults with hypermobile Ehlers-Danlos syndrome / hypermobility spectrum disorders and shoulder symptoms: a systematic review. Arch Rehabil Res Clin Transl. 2024;6(3):100360. doi:10.1016/j.arrct.2024.100360
- Brittain MG, Flanagan SC, Foreman LN, Teran-Wodzinski P. Physical therapy interventions in generalized hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome: a scoping review. Disabil Rehabil. 2023;45(24):4017 to 4031. doi:10.1080/09638288.2023.2216028
- Bathen T, Hångmann AB, Hoff M, Andersen LØ, Rand-Hendriksen S. Multidisciplinary treatment of disability in Ehlers-Danlos syndrome hypermobility type: a pilot study using physical and cognitive-behavioural therapy on 12 women. Am J Med Genet A. 2013;161A(12):3005 to 3011. doi:10.1002/ajmg.a.36060
- Buryk-Iggers S, Mittal N, Santa Mina D, Adams SC, Englesakis MF, Rachinsky M, Lopez-Hernandez L, Hussey L, McGillis L, McLean L, Laflamme C, Rozenberg D, Clarke H. Exercise and rehabilitation in people with Ehlers-Danlos syndrome: a systematic review. Arch Rehabil Res Clin Transl. 2022;4(2):100189. doi:10.1016/j.arrct.2022.100189
Additional references: Foot Arches
Sourced from Foot Arches. These references support the deeper discussion in the linked blog.
- Akkaya KU, Burak M, Yildiz R, Yildiz A, Elbasan B. Examination of foot sensations in children with generalized joint hypermobility. Early Human Development. 2023;180:105755. doi: 10.1016/j.earlhumdev.2023.105755
- Camerota F, Galli M, Cimolin V, Celletti C, Ancillao A, Blow D, Albertini G. The effects of neuromuscular taping on gait walking strategy in a patient with joint hypermobility syndrome/Ehlers-Danlos syndrome hypermobility type. Therapeutic Advances in Musculoskeletal Disease. 2015;7(1):3-10. doi: 10.1177/1759720X14564561
- Dupuy EG, Leconte P, Vlamynck E, Sultan A, Chesneau C, Denise P, Besnard S, Bienvenu B, Decker LM. Ehlers-Danlos Syndrome, Hypermobility Type: Impact of Somatosensory Orthoses on Postural Control (A Pilot Study). Frontiers in Human Neuroscience. 2017;11:283. doi: 10.3389/fnhum.2017.00283
- Kim EK, Kim JS. The effects of short foot exercises and arch support insoles on improvement in the medial longitudinal arch and dynamic balance of flexible flatfoot patients. Journal of Physical Therapy Science. 2016;28(11):3136-3139. doi: 10.1589/jpts.28.3136
- Mulligan EP, Cook PG. Effect of plantar intrinsic muscle training on medial longitudinal arch morphology and dynamic function. Manual Therapy. 2013;18(5):425-430. doi: 10.1016/j.math.2013.02.007
- Vermeulen S, De Mits S, De Ridder R, Calders P, De Schepper J, Malfait F, Rombaut L. Altered multisegment ankle and foot kinematics during gait in patients with hypermobile Ehlers-Danlos syndrome/hypermobility spectrum disorder: a case-control study. Arthritis Care and Research. 2022;74(5):841-848. doi: 10.1002/acr.24526
- Lynn SK, Padilla RA, Tsang KK. Differences in static- and dynamic-balance task performance after 4 weeks of intrinsic-foot-muscle training: the short-foot exercise versus the towel-curl exercise. Journal of Sport Rehabilitation. 2012;21(4):327-333. doi: 10.1123/jsr.21.4.327
- Sung PS, Zipple JT, Andraka JM, Danial P. The kinetic and kinematic stability measures in healthy adult subjects with and without flat foot. The Foot. 2017;30:21-26. doi: 10.1016/j.foot.2017.01.010
- Tahmasebi R, Karimi MT, Satvati B, Fatoye F. Evaluation of standing stability in individuals with flatfeet. Foot and Ankle Specialist. 2014;8(3):168-174. doi: 10.1177/1938640014557075
- Moon D, Jung J. Effect of incorporating short foot exercises in the balance rehabilitation of flat foot: a randomized controlled trial. Healthcare. 2021;9(10):1358. doi: 10.3390/healthcare9101358
- Cheng J, Han D, Qu J, et al. Effects of short foot training on foot posture in patients with flatfeet: a systematic review and meta-analysis. Journal of Back and Musculoskeletal Rehabilitation. 2024;37(4):857-872. doi: 10.3233/BMR-230226
- Burns J, Crosbie J, Hunt A, Ouvrier R. The effect of pes cavus on foot pain and plantar pressure. Clinical Biomechanics. 2005;20(9):877-882. doi: 10.1016/j.clinbiomech.2005.03.006
- Burns J, Crosbie J. Weight bearing ankle dorsiflexion range of motion in idiopathic pes cavus compared to normal and pes planus feet. The Foot. 2005;15(2):91-94. doi: 10.1016/j.foot.2005.03.003
- Williams DS 3rd, McClay IS, Hamill J. Arch structure and injury patterns in runners. Clinical Biomechanics. 2001;16(4):341-347. doi: 10.1016/S0268-0033(01)00005-5
- Smith TO, Jerman E, Easton V, Bacon H, Armon K, Poland F, Macgregor AJ. Do people with benign joint hypermobility syndrome (BJHS) have reduced joint proprioception? A systematic review and meta-analysis. Rheumatology International. 2013;33(11):2709-2716. doi: 10.1007/s00296-013-2790-4
- Kennedy PM, Inglis JT. Distribution and behaviour of glabrous cutaneous receptors in the human foot sole. The Journal of Physiology. 2002;538(3):995-1002. doi: 10.1113/jphysiol.2001.013087
- Robbins S, Gouw GJ, McClaran J. Shoe sole thickness and hardness influence balance in older men. Journal of the American Geriatrics Society. 1992;40(11):1089-1094. doi: 10.1111/j.1532-5415.1992.tb01795.x
For why we don’t build the rehab framework around fascia release or “fascia training”, the long version of that argument is here: Fascia and hypermobility, what the research actually says.