
Last updated May 2026
Key Takeaways
- Hypermobility exists on a spectrum from asymptomatic flexibility to symptomatic conditions including hypermobility spectrum disorder (HSD) and hypermobile Ehlers-Danlos syndrome (hEDS).
- There is currently no genetic test for hEDS. Diagnosis uses the 2017 international criteria combining the Beighton Score with systemic features of connective tissue involvement.
- Common comorbidities include POTS, mast cell activation syndrome (MCAS), autism and ADHD, anxiety, gastrointestinal dysfunction, and endometriosis.
- Proprioceptive training and isometric strengthening are the most evidence-supported exercise approaches. Traditional static stretching is generally counterproductive for hypermobile joints.
- Research shows a strong association between joint hypermobility and anxiety disorders, likely related to altered autonomic nervous system function.
You have been told your joints are “just a bit hypermobile.” Or maybe you have been handed a diagnosis of hEDS and left to Google it on your own. Either way, you are probably dealing with a body that does not quite work the way everyone else’s seems to, with pain that is hard to explain, fatigue that does not respond to sleep, and a string of symptoms that do not seem connected on the surface but somehow all live in the same person.
That is not coincidence. It is connective tissue.
This is your starting point. We have pulled together everything you need to know about hypermobility and Ehlers-Danlos syndrome into one place. Each section expands when you click it, and links to a deeper article if you want to go further. Pick the topics that matter to you and skip what does not.

Looking for the exercise side of all this?
If you want the practical movement and rehab piece, the companion guide goes deep on what works, what does not, joint by joint videos, taping, motor learning, foot arches, the lot. It is the most useful place to start if pain and instability are the main issues.
What Is Hypermobility?
Hypermobility sits on a spectrum. For some it is nothing more than a physical trait. For others it brings pain, instability, fatigue and a long list of systemic symptoms. The difference matters, and so do the categories used to describe it.
Read MoreHypermobility means your joints move beyond the range that is typical for your age and sex. That is the simple version. The more useful version is that hypermobility sits on a spectrum, running from completely asymptomatic (the gymnast who never has a bad day) all the way to a connective tissue disorder that affects multiple body systems simultaneously.
Generalised joint hypermobility (GJH) is common. Depending on the population studied, estimates range widely, and it tends to decrease with age and is more prevalent in females and in people of South Asian and African descent. For many it is nothing more than a physical trait. The trouble starts when hypermobility comes with pain, instability, fatigue, autonomic symptoms, or other features that make daily life significantly harder [1,2].
When it comes to categorising where on that spectrum someone sits, the 2017 International Classification of the Ehlers-Danlos Syndromes is the current reference point [1]. It split the hypermobility world into two main categories that get confused constantly.
Hypermobility Spectrum Disorder (HSD)
HSD is diagnosed in people who have symptomatic joint hypermobility, meaning it is causing real musculoskeletal problems, but who do not fully meet the clinical criteria for hEDS [2]. It is not a lesser condition, it is a separate diagnostic category. The symptoms, impact on quality of life, and comorbidities can be just as significant as in hEDS [19]. HSD replaced the old term “benign joint hypermobility syndrome,” and the word “benign” was rightly dropped. There is nothing benign about chronic pain and instability [18].
Hypermobile Ehlers-Danlos Syndrome (hEDS)
hEDS is the most common subtype of EDS. It is characterised by generalised joint hypermobility combined with a specific cluster of additional features: systemic connective tissue involvement, a positive family history, and the absence of conditions that would otherwise explain the symptoms [1]. Unlike the other 12 EDS subtypes, hEDS has no identified genetic marker. It cannot be confirmed or ruled out through a blood test, which creates significant diagnostic challenges [3].
Together, hEDS and HSD are far more common than most clinicians are taught. Population data suggests their combined prevalence is likely greater than 1 in 500 [4]. Some estimates put it considerably higher. For context, this makes the hEDS/HSD group one of the most common underdiagnosed connective tissue conditions in clinical practice.
It is also worth being clear about something that trips people up: you can have hypermobility without feeling or looking flexible. The internal laxity of connective tissue does not always translate to the splits on demand.
→ Read whether you can be hypermobile without looking flexible
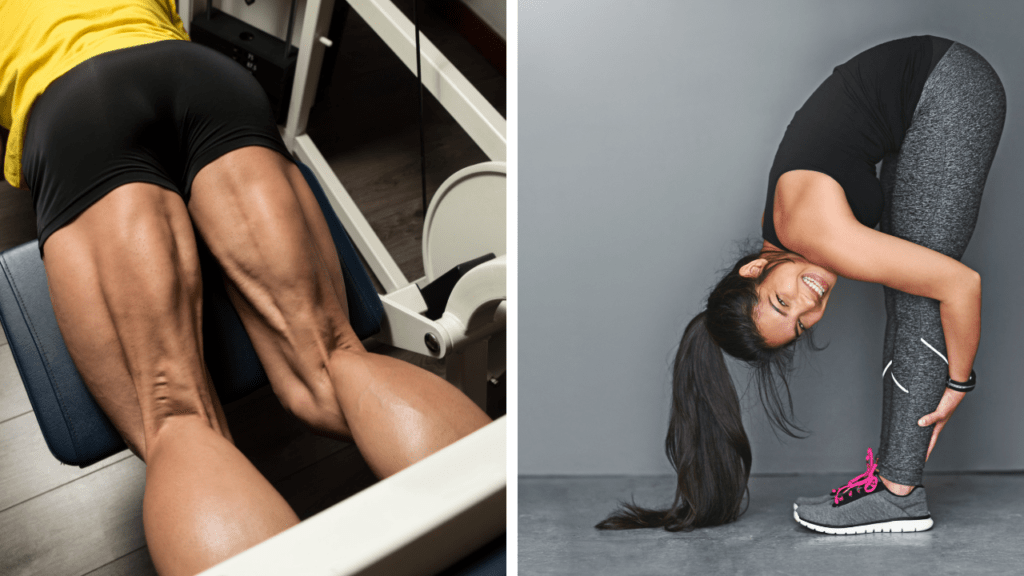
Exercise and Movement
Exercise is one of the most powerful tools for managing hypermobility, and one of the most mismanaged. The default advice to rest more when joints hurt is often exactly wrong. The wrong type of exercise, on the other hand, can genuinely make things worse.
Read MoreDeconditioning worsens joint instability, amplifies pain sensitivity, and accelerates the downward spiral that many find themselves in. End-range loading, heavy ballistic movements, and anything that exploits the existing laxity rather than building stability around it tends to make things worse. The fundamentals of exercise for hypermobility lay out the framework that works.
Stretching: Less Than You Think
This is one of the most counter-intuitive aspects of managing hypermobility: the joints are already too mobile. Most people do not need more range. They need better control through the range they have got. Passive stretching, particularly into end range, often loads already compromised tissue and can increase instability over time. The truth about stretching in hypermobility explains the evidence and what to do instead. The same logic applies to the two practices most commonly recommended to hypermobile people: see our full reviews of what the evidence actually shows for Pilates in hypermobility and fibromyalgia and what the evidence shows for yoga in chronic pain and hypermobility.
Core Stability and Proprioceptive Training
Given that proprioceptive impairment is a key feature of hypermobility, exercises that specifically train joint position sense and neuromuscular control are particularly valuable. Graduated loading, stability work, and proprioceptive re-training tend to produce better outcomes than generic gym programmes. See our piece on core exercises for hypermobility for the practical version.
KT Tape and Supports
Taping can be a useful adjunct for joint stability, particularly during periods of flare or when specific joints are repeatedly subluxing. How to use KT tape in hypermobility and EDS covers application and evidence.
→ Read the full exercise and rehabilitation guide for hypermobility
Types of EDS: A Quick Overview

The 2017 international classification recognised 13 subtypes of EDS, each with its own clinical features and, in most cases, an identified genetic cause. For most people reading this, hEDS is the relevant one. Here is the rest of the picture.
Read MoreThe 2017 international classification recognised 13 subtypes of EDS, each with its own clinical features, inheritance pattern, and in most cases, an identified genetic cause [1]. Here is a brief overview:
| Type | Key Features | Genetic Basis |
|---|---|---|
| Hypermobile (hEDS) | Joint hypermobility, musculoskeletal pain, skin involvement (minor), dysautonomia | Unknown |
| Classical | Skin hyperextensibility, atrophic scarring, joint hypermobility | COL5A1/COL5A2 (type V collagen) |
| Vascular (vEDS) | Arterial/organ rupture, thin translucent skin (life-threatening) | COL3A1 (type III collagen) |
| Kyphoscoliotic | Progressive scoliosis, muscle hypotonia, ocular fragility | PLOD1, FKBP14 |
| Arthrochalasia | Severe joint hypermobility, bilateral hip dislocations at birth | COL1A1, COL1A2 |
| Dermatosparaxis | Extreme skin fragility, drooping skin, hernias | ADAMTS2 |
| Classical-like | Similar to classical but without atrophic scarring | TNXB |
| Cardiac-valvular | Cardiac valve problems, skin and joint involvement | COL1A2 (recessive) |
| Spondylodysplastic | Short stature, muscle hypotonia, bowing of limbs | B4GALT7, B3GALT6, SLC39A13 |
| Musculocontractural | Congenital contractures, craniofacial features, progressive scoliosis | CHST14, DSE |
| Myopathic | Muscle hypotonia/atrophy, proximal joint contractures | COL12A1 |
| Periodontal | Severe periodontitis, pretibial plaques, joint laxity | C1R, C1S |
| Brittle Cornea Syndrome | Corneal rupture risk, keratoconus, blue sclera | ZNF469, PRDM5 |
For most people reading this, hEDS is the relevant type. Vascular EDS is worth knowing about because it is the most serious and carries risks of arterial and organ rupture. If there is a family history of unexplained early cardiovascular events or bowel perforations, vascular EDS should be discussed with a genetics specialist.
The other 11 subtypes are genuinely rare. hEDS accounts for the vast majority of EDS cases seen in clinical practice, followed by classical EDS [13].
→ Read what the 2026 EDS classification update means for you
How Is Hypermobility and EDS Diagnosed?

Diagnosis is clinical. There is no blood test for hEDS, no scan, no single sign that confirms or rules it out. What there is is a structured set of criteria, a flawed but useful scoring system, and a long history of misclassification.
Read MoreFor most EDS subtypes, genetic testing can confirm or rule out a diagnosis. For hEDS, there is currently no genetic test available [1,3]. The 2017 international criteria are the current reference point.
The Beighton Score
The Beighton score is a 9-point scale used to measure generalised joint hypermobility. It tests five movements: forward spinal flexion (palms flat on floor with knees straight), plus four bilateral movements: hyperextension of the fifth finger beyond 90°, thumb to forearm, elbow hyperextension beyond 10°, and knee hyperextension beyond 10°. Each bilateral movement scores 1 point per side, the spinal test scores 1 point.
A Beighton score of 5 or more (in adults under 50) is used as one criterion for hEDS diagnosis. A score of 4 may also be sufficient in older adults. But it is worth understanding what the Beighton score is and is not. The score has real limitations, missing hypermobility in the hips, shoulders, ankles, and jaw. Plenty of people with significant systemic hypermobility score low, particularly if they have developed protective muscle tension or are older. The score was never designed as a standalone diagnostic tool, yet it is often used as one.
The 2017 hEDS Criteria
The 2017 diagnostic criteria for hEDS require three things to all be present:
- Criterion 1: Generalised joint hypermobility (meeting age/sex-specific Beighton thresholds, or a positive five-part questionnaire result)
- Criterion 2: Two or more of three feature groups: Feature A (systemic connective tissue manifestations including skin involvement, marfanoid features, stretch marks, hernia, pelvic floor dysfunction, dental crowding or palatal abnormalities); Feature B (positive family history, first-degree relative with confirmed hEDS); Feature C (musculoskeletal complications including at least three of musculoskeletal pain, recurrent joint dislocations, joint instability, etc.)
- Criterion 3: Exclusion of other heritable connective tissue disorders and conditions explaining the hypermobility
This is a more demanding criteria set than its predecessor, which means some people previously diagnosed with hEDS now fall into HSD. That is not a demotion. It is a more precise classification. The management approach is largely the same [18].
For a full walkthrough of the diagnostic process, this guide on how hypermobility and EDS are diagnosed covers it step by step. If other conditions could explain your symptoms, it is also worth reading about what can be mistaken for hypermobility.
→ Read the step-by-step guide on how hypermobility and EDS are diagnosed
Common Symptoms Beyond Flexible Joints

This is the section that tends to land hardest for people who have spent years being told their only issue is bendy joints. hEDS and HSD are systemic conditions, and the symptoms reflect that.
Read MoreThe connective tissue that is behaving differently runs through virtually every structure in the body, which means symptoms can show up almost anywhere. The full symptom picture in hEDS and HSD is broader than most clinicians expect. Here are the main areas.
Chronic Pain
Chronic widespread pain is among the most common and most disabling features of hEDS and HSD [4,15]. It tends to be multifactorial. Joint instability causes microtrauma, but there is also evidence of altered central pain processing, reduced pain thresholds, and impaired conditioned pain modulation [15]. This is why straightforward pain-relief approaches often do not work well. The pain is not just coming from damaged joints. Understanding the mechanisms behind chronic pain in hypermobility is important before choosing how to address it.
For a comprehensive look at what the research says about different pain medications for this population, including NSAIDs, gabapentinoids, opioids, LDN, and local anaesthetic resistance, see our guide to pain medication for hypermobility and EDS.
Fatigue
Fatigue that does not respond to rest is one of the most reported symptoms and one of the hardest to explain to others. It is not laziness, it is physiological. The body’s constant effort to compensate for unstable joints, the disrupted sleep that often accompanies pain, the autonomic dysfunction, the deconditioning cycle. It all adds up. Hypermobility is detected in 30 to 57% of patients with ME/CFS and fibromyalgia, suggesting significant overlap in the underlying mechanisms [13].
Gastrointestinal Issues
GI symptoms are extraordinarily common. Research comparing hEDS/HSD patients to controls found abdominal pain in 69% (versus 27% of controls), constipation in 73% (versus 16%), and diarrhoea in 47% (versus 9%) [10]. The causes are multiple: connective tissue laxity in the gut wall itself, autonomic dysfunction affecting motility, mast cell involvement, and the side effects of medications. Delayed gastric emptying (gastroparesis) is increasingly being recognised as a feature [21]. This matters more now that GLP-1 receptor agonists like Ozempic, Wegovy and Mounjaro are widely prescribed, since those drugs slow the gut further as part of how they work, which is something anyone with EDS considering Ozempic needs to factor into the conversation with their doctor. We have written about why constipation in hypermobility is not a fibre problem and the evidence-based approach to it, including the rectal hyposensitivity finding that explains why standard advice so often fails.
POTS and Dizziness
Postural orthostatic tachycardia syndrome, or POTS, is a form of dysautonomia in which the heart rate increases by more than 30 beats per minute on standing (or exceeds 120 bpm), often accompanied by lightheadedness, brain fog, nausea, and near-fainting. It is closely linked to hypermobility. 31% of POTS patients met full criteria for hEDS in one study using the 2017 criteria, with a further 24% having generalised joint hypermobility (GJH) without meeting full hEDS criteria. In total, 55% of the POTS cohort had some form of GJH [5]. The likely mechanism is that lax connective tissue allows excessive venous pooling in the legs on standing, reducing cardiac return and triggering compensatory tachycardia [21].
Brain Fog
Cognitive difficulties including concentration problems, word-finding difficulties, and difficulty processing information are widely reported. The causes are not fully understood but are thought to involve cerebral blood flow reductions secondary to POTS, disrupted sleep, the neurological effects of chronic pain, and possibly direct neurological involvement. A detailed look at brain fog in EDS and POTS covers this in full.
Anxiety
Those with hypermobility have a significantly elevated risk of anxiety disorders. The relationship is not simply psychological. It is physiological. Joint hypermobility syndrome at age 18 was associated with an adjusted odds ratio of 3.14 for anxiety disorder in a large cohort study, with the effect mediated by autonomic factors including elevated resting heart rate [9]. The body’s threat-detection systems are genuinely more active. Why anxiety is wired into hypermobility at a physiological level is one of the most important things to understand.
Sleep Problems
Poor sleep is near-universal in hEDS and HSD. Pain makes it hard to find a comfortable position, autonomic dysregulation can cause night-time heart rate spikes, and anxiety interferes with both falling and staying asleep. The full picture of sleep in hypermobility covers both the causes and practical approaches.
Skin and Wound Healing
Skin features in hEDS can be subtle, but many people notice unusually soft or velvety skin, easy bruising, slow wound healing, or pronounced stretch marks. The collagen dysfunction that underpins EDS affects skin structure. Interestingly, the same collagen differences may mean those with hypermobility often appear younger than their age.
Headaches and Migraines
Head pain is one of the most common and most misunderstood problems in this group. The label “hypermobility headache” describes who is getting the headache, not what is causing it. The top three levels of the neck feed into the same brainstem relay as the trigeminal nerve, so an irritable or poorly controlled upper neck can produce pain felt right across the head and face. Several very different mechanisms wear the same coat here, including migraine, cervicogenic headache from the upper neck, the low-pressure headache that eases when you lie flat, jaw-driven pain, and the medication-overuse trap. They feel similar from the inside but need completely different first moves, which is why generic headache advice so often does nothing. Splitting the mechanisms apart is the first step to matching the right approach to the right cause.
The Science: What Is Actually Going Wrong

When it comes to understanding why hEDS and HSD cause so many wide-ranging symptoms, the answer starts with connective tissue and branches out from there, through proprioception and into the autonomic nervous system.
Read MoreCollagen and the Extracellular Matrix
Connective tissue is the structural framework of the body. It holds joints together, supports organ walls, forms the scaffolding within skin, lines blood vessels, and more. Its primary structural protein is collagen, and the rest of the extracellular matrix (ECM): fibronectin, elastin, tenascin, proteoglycans. All of it works with collagen to give tissue its mechanical properties [3,14].
In the genetically confirmed EDS subtypes, there are known mutations affecting collagen biosynthesis, cross-linking, or assembly. The 2017 classification identified 13 subtypes, and across them around 20 causal genes have now been described [3]. In hEDS, no causative gene has been found, but research consistently shows ECM disorganisation in patient tissue. One 2024 study found a distinctive fragmentation pattern in fibronectin, type I collagen, and tenascin in plasma from hEDS and HSD patients, supporting the hypothesis that both conditions share a common ECM disruption even without an identified genetic cause [16].
Questions remain about whether those with hypermobility have less collagen overall, or whether the collagen they have is structurally different. The research on collagen in hypermobility goes into this in detail.
Proprioception: The Body’s Sixth Sense
Proprioception is the body’s ability to sense its own position in space. It depends on mechanoreceptors, sensory neurons embedded in joint capsules, tendons, and muscles, feeding signals back to the brain. In symptomatic hypermobility, this system is compromised. The loose, compliant connective tissue surrounding joints reduces the precision of position sensing, contributing to poor coordination, a tendency to misjudge joint position, and elevated injury risk.
This proprioceptive impairment is not trivial. It partly explains why chronic pain develops in hypermobility. The brain receives inconsistent and imprecise sensory signals from joints that are moving in uncontrolled ways, and the nervous system escalates its alarm responses accordingly. The result is a pain system that has been sensitised over years of sub-optimal mechanical feedback.
The Autonomic Nervous System
The autonomic nervous system controls unconscious body functions: heart rate, blood pressure, digestion, sweating, breathing. In hEDS and HSD, autonomic dysfunction is common. The mechanisms are thought to include the mechanical effects of lax connective tissue on blood vessels (reducing venous return), altered baroreceptor function, and possible neurological involvement [8,21].
This is why POTS, GI dysmotility, temperature dysregulation, and anxiety can all appear in the same person. They share an autonomic root. It also connects to how the brain and body interact in chronic illness.
→ Read more on what the research says about collagen in hypermobility
Comorbidities: What Tends to Travel With Hypermobility

One of the most consistent findings in hEDS and HSD research is the sheer number of conditions that co-occur. These are not coincidences. They reflect shared underlying biology.
Read MorePOTS (Postural Orthostatic Tachycardia Syndrome)
POTS and hypermobility are closely linked. In one study, 31% of POTS patients met criteria for hEDS, and a further 24% had GJH without the full diagnosis, meaning 55% of the cohort had some form of generalised joint hypermobility [5]. The connection runs in both directions. Exercise management for POTS requires a specific approach, and the evidence on salt in POTS management is more complex than many guides suggest.
Mast Cell Activation Syndrome (MCAS)
MCAS involves inappropriate mast cell degranulation, triggering allergic-type responses (flushing, hives, GI symptoms, anaphylactic reactions) in the absence of a clearly identifiable allergen. The association with hEDS is clinically well-recognised [11]. The biological mechanism is not fully established, but the close co-occurrence of hEDS, POTS, and MCAS (sometimes called the “triad”) is widely reported in clinical settings. What you need to know about MCAS covers diagnosis and management.
Autism and ADHD
The neurodevelopmental connections to hypermobility are real and increasingly well-documented. In a nationwide Swedish cohort study, EDS was associated with an autism risk ratio of 7.4 and an ADHD risk ratio of 5.6 compared to the general population [6]. A retrospective study of children with HSD/hEDS found 16% had a confirmed ADHD diagnosis, with a further 7% under investigation [7]. A separate study found that neurodivergent adults had a GJH prevalence of roughly 51% versus approximately 20% in the general population, and joint hypermobility mediated the link between neurodivergence and both dysautonomia and pain [8].
This is not well understood yet, but the overlap appears to involve shared genetic pathways, proprioceptive processing differences, and autonomic dysfunction [6,8]. The research on hypermobility and autism looks at this in more detail, as does what neuroscience tells us about brain differences in ASD and ADHD.
Depression and Anxiety
Beyond the direct physiological mechanisms, those with hypermobility face elevated rates of depression. EDS is associated with a 3.4-fold increased risk of depression and a 2.1-fold increased risk of suicide attempt in population-level data [6]. Joint hypermobility syndrome at age 18 was associated with a 3.53-fold increase in depressive disorder [9]. This is not just a reaction to living with a difficult condition. It reflects genuine neurobiological overlap, including autonomic dysregulation, altered interoception, and the psychological effects of years of unvalidated symptoms [9].
Endometriosis and Gynaecological Issues
Those with hEDS have significantly higher rates of gynaecological symptoms. In a cohort of 386 women with hEDS, 76% reported menorrhagia, 72% dysmenorrhoea, 43% dyspareunia, and 28% had experienced spontaneous abortion [12]. The connection to endometriosis requires careful interpretation. hEDS symptoms can closely mimic endometriosis and the two can co-occur. Awareness of this helps avoid unnecessary surgery [12]. The link between EDS and endometriosis explores the latest thinking.
Scoliosis and Structural Issues
Spinal curvature is more common in hypermobility, partly because joint laxity affects the support structures around the spine. The relationship between scoliosis and hypermobility covers what to look for and how it affects management.
Pregnancy with EDS or hypermobility raises specific considerations around connective tissue changes, anaesthesia, labour, and postpartum recovery. Our detailed guide to EDS, hypermobility, and pregnancy covers everything from preconception planning through to breastfeeding and the 2024 expert guidelines.
Weight Changes
Both unexplained weight gain and unintentional weight loss are reported in hEDS. GI dysmotility can affect absorption and appetite, medications have metabolic effects, and reduced activity due to pain and fatigue affects energy balance. How EDS affects body weight looks at the evidence. There is also a related question around whether losing weight increases subluxation risk in hypermobility.
Nutrition and Supplements

Nutrition in hypermobility does not have a definitive prescription, but there are evidence-informed principles worth following and a few supplements that have attracted enough research to be worth considering.
Read MoreDiet
When it comes to eating with hEDS or HSD, the main goals are reducing systemic inflammation, supporting connective tissue health, and managing any GI comorbidities that affect absorption. An anti-inflammatory diet is the most commonly cited approach, and the full evidence-based guide to diet in hypermobility covers what that actually means in practice, beyond generic advice. Mast cell considerations may also affect food choices in those with MCAS comorbidity, and FODMAP management is sometimes relevant for those with significant GI symptoms.
Creatine
Creatine is one of the most robustly studied supplements in exercise science and has a plausible case for benefit in hypermobility. It supports phosphocreatine resynthesis in muscles, improves high-intensity exercise capacity, and may support connective tissue health through its effects on muscle function and reduced fatigue during training. The evidence for creatine in hypermobility and EDS looks specifically at what the research supports and how to use it effectively.
Vitamin C, magnesium, and omega-3 fatty acids are also commonly discussed in this context, though the evidence base is thinner. The key is matching any supplementation strategy to your individual symptom profile.
→ Read the full evidence-based guide to diet in hypermobility
Daily Living: Sleep, Pacing, and Flare Management
Living with hEDS or HSD is not just about medical appointments and treatment plans. A lot of the day-to-day management comes down to patterns: sleep, activity pacing, and having a sensible strategy when things get worse.
Read MoreSleep
Poor sleep is one of the biggest drivers of the pain-fatigue cycle in hypermobility. Pain disrupts sleep, poor sleep lowers pain thresholds, which increases pain, and so on. Getting sleep architecture right, not just time in bed but sleep quality, matters significantly. Understanding sleep in hypermobility covers the causes and practical strategies in detail, including the roles of positioning, autonomic function, and the anxiety overlap.
Pacing
Pacing is the practice of managing activity levels to avoid boom-and-bust cycles, specifically periods of doing too much followed by crashes that can last days or weeks. It is not about doing less; it is about distributing energy and load more evenly. The evidence-based pacing guide for EDS and chronic pain is the place to start.
Flare Management
Flares are periods of increased symptoms: more pain, more fatigue, more instability. They can be triggered by physical overexertion, illness, stress, hormonal fluctuation, or sometimes nothing identifiable at all. Having a pre-planned response matters more than reacting to each flare from scratch. Managing EDS flare-ups covers what tends to help and what does not.
→ Read the evidence-based pacing guide for EDS and chronic pain
Does Hypermobility Get Worse With Age?

Joint hypermobility itself tends to decrease with age as connective tissue stiffens. The lived condition is more complicated than that, and the trajectory is not uniformly negative.
Read MoreSo in one sense, older people with hypermobility may become less hypermobile by the numbers. But that does not mean the condition becomes easier to live with. The cumulative effects of years of joint instability, repeated microtrauma, and chronic pain can mean that symptoms become more entrenched over time even as the Beighton score drops. Comorbidities may accumulate. The deconditioning cycle, if unchecked, can have significant long-term consequences.
The picture is also highly individual, and it is not uniformly negative. People who get good support early, who find the right exercise approach, and who manage the autonomic and sleep components often report meaningful improvements in quality of life. It is not a single direction. A detailed look at ageing with EDS goes through what the evidence actually shows.
Getting the Right Support
One of the most consistent themes in hEDS and HSD is the difficulty of getting appropriate medical care. Diagnostic delays of a decade or more are common, and the mismatch between how disabling these conditions can be and how they are often treated is a real problem.
Read MoreMany patients have their symptoms attributed to anxiety, hypochondria, or deconditioning before a connective tissue problem is even considered.
Medical Trauma
Being dismissed, disbelieved, or mismanaged over years creates a particular kind of damage that sits alongside the physical condition itself. The impact of medical trauma in EDS addresses this directly, covering both the experience and what recovery from it can look like. This matters because medical trauma can make people reluctant to engage with practitioners even when good support is available.
Finding Practitioners Who Understand
Not all physiotherapists, GPs, or specialists have working knowledge of hEDS and HSD. This is not entirely their fault. It is not well covered in standard medical training, but it does mean that navigating the healthcare system requires some self-advocacy. Key things to look for in a physiotherapist: understanding that end-range loading is problematic, focus on stability and neuromuscular control rather than passive stretching, awareness of the autonomic and fatigue components, and experience with hypermobility patients specifically.
The same principles apply to other professionals. A pain specialist who does not understand central sensitisation in connective tissue disorders, or a cardiologist who dismisses POTS as anxiety, is likely to cause more harm than good regardless of their individual expertise.
The Right Mental Model
Perhaps the most useful reframe for anyone newly diagnosed: this is a manageable condition, not a terminal one. The research on exercise response, pacing, and structured rehabilitation is genuinely encouraging. The challenge is finding the right level of support and building a management strategy that addresses the whole picture, not just one joint at a time.
Chronic Pain, Relationships and Intimacy

The bit of chronic pain that gets skipped in clinic is the bit that affects your relationship, your sex life, and how you talk about any of it with the person you share a bed with. Sleep gets asked about. Walking the dog gets asked about. The fact your hip subluxes when you change position, or that you crash for three days after anything more than a cuddle, somehow does not.
That gap is where most of the hidden suffering sits, and it shows up across hypermobility, fibromyalgia, POTS and ME/CFS. We have a full guide covering disclosure to new partners, communication inside long term relationships, positioning, pacing intimacy, the LGBTQ and polyamorous experience of chronic pain, and how to look after a body that does not always cooperate.
→ Read the full guide: Chronic Pain, Relationships and Intimacy
Where to Go From Here
If you have made it this far, you probably know more about your own condition than most of the people you have seen about it. And that is not a dig at them, it is just the reality of how little time hypermobility gets in training.
Now, if you want to actually start doing something with all of this, we have built a few things that might help. The Hypermobility Live Workshop is four weeks of us breaking down the frameworks we use in our studios, with live Q&A so you can ask about your specific situation. Or if you would rather go at your own pace, have a look through the course library, there is stuff in there covering everything from joint stability to pacing to making sense of your nervous system.
And if you just want free stuff to get started, the Hypermobility Exercise and Rehabilitation Guide has exercises, taping videos, and practical bits you can use straight away.

Ready to work through this with structure and support?
The Hypermobility Live Workshop is four weeks of breaking down the frameworks we use in our studios, with live Q&A so you can ask about your specific situation. Two free courses are included.
References
- Malfait F, Francomano C, Byers P, et al. (2017) The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):8-26. doi: 10.1002/ajmg.c.31552
- Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A. (2017) A framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin Med Genet. 2017;175(1):148-157. doi: 10.1002/ajmg.c.31539
- Ritelli M, Colombi M. (2020) Molecular Genetics and Pathogenesis of Ehlers-Danlos Syndrome and Related Connective Tissue Disorders. Genes. 2020;11(5):547. doi: 10.3390/genes11050547
- Hakim A, Tinkle B, Francomano C. (2021) Ehlers-Danlos syndromes, hypermobility spectrum disorders, and associated co-morbidities: Reports from EDS ECHO. Am J Med Genet C Semin Med Genet. 2021;187(4):413-415. doi: 10.1002/ajmg.c.31954
- Miller AJ, Stiles LE, Sheehan T, Bascom R, Levy HP, Francomano CA, Robertson D, Hendrickson AG, Arnold AC. (2020) Prevalence of hypermobile Ehlers-Danlos syndrome in postural orthostatic tachycardia syndrome. Auton Neurosci. 2020;224:102637. doi: 10.1016/j.autneu.2020.102637
- Cederlöf M, Larsson H, Lichtenstein P, Almqvist C, Serlachius E, Ludvigsson JF. (2016) Nationwide population-based cohort study of psychiatric disorders in individuals with Ehlers-Danlos syndrome or hypermobility syndrome and their siblings. BMC Psychiatry. 2016;16:207. doi: 10.1186/s12888-016-0922-6
- Kindgren E, Quiñones Perez A, Knez R. (2021) Prevalence of ADHD and Autism Spectrum Disorder in Children with Hypermobility Spectrum Disorders or Hypermobile Ehlers-Danlos Syndrome: A Retrospective Study. Neuropsychiatr Dis Treat. 2021;17:379-388. doi: 10.2147/NDT.S290494
- Csecs JLL, Iodice V, Rae CL, Brooke A, Simmons R, Quadt L, Savage GK, Dowell NG, Prowse F, Themelis K, Mathias CJ, Critchley HD, Eccles JA. (2022) Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. Front Psychiatry. 2022;12:786916. doi: 10.3389/fpsyt.2021.786916
- Eccles JA, Quadt L, McCarthy H, et al. (2022) Variant connective tissue (joint hypermobility) and its relevance to depression and anxiety in adolescents: a cohort-based case-control study. BMJ Open. 2022;12:e066130. doi: 10.1136/bmjopen-2022-066130
- Thwaites PA, Gibson PR, Burgell RE. (2022) Hypermobile Ehlers-Danlos syndrome and disorders of the gastrointestinal tract: What the gastroenterologist needs to know. J Gastroenterol Hepatol. 2022;37(9):1693-1709. doi: 10.1111/jgh.15927
- Yao L, Subramaniam K, Raja KM, et al. (2025) Association of postural orthostatic tachycardia syndrome, hypermobility spectrum disorders, and mast cell activation syndrome in young patients; prevalence, overlap and response to therapy depends on the definition. Front Neurol. 2025;16:1513199. doi: 10.3389/fneur.2025.1513199
- Hugon-Rodin J, Lebègue G, Becourt S, Hamonet C, Gompel A. (2016) Gynecologic symptoms and the influence on reproductive life in 386 women with hypermobility type Ehlers-Danlos syndrome: a cohort study. Orphanet J Rare Dis. 2016;11(1):124. doi: 10.1186/s13023-016-0511-2
- Ganesh R, Munipalli B. (2024) Long COVID and hypermobility spectrum disorders have shared pathophysiology. Front Neurol. 2024;15:1455498. doi: 10.3389/fneur.2024.1455498
- Malek S, Köster DV. (2021) The Role of Cell Adhesion and Cytoskeleton Dynamics in the Pathogenesis of the Ehlers-Danlos Syndromes and Hypermobility Spectrum Disorders. Front Cell Dev Biol. 2021;9:649082. doi: 10.3389/fcell.2021.649082
- Malfait F, Colman M, Vroman R, De Wandele I, Rombaut L, Miller RE, Malfait AM, Syx D. (2021) Pain in the Ehlers-Danlos syndromes: Mechanisms, models, and challenges. Am J Med Genet C Semin Med Genet. 2021;187(4):429-445. doi: 10.1002/ajmg.c.31950
- Ritelli M, Chiarelli N, Cinquina V, et al. (2025) Bridging the Diagnostic Gap for Hypermobile Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorders: Evidence of a Common Extracellular Matrix Fragmentation Pattern in Patient Plasma as a Potential Biomarker. Am J Med Genet A. 2025;197(1):e63857. doi: 10.1002/ajmg.a.63857
- Morlino S, Castori M. (2023) Placing joint hypermobility in context: traits, disorders and syndromes. Br Med Bull. 2023;147(1):90-107. doi: 10.1093/bmb/ldad013
- Carroll M. (2023) Hypermobility spectrum disorders: A review. Rheumatol Immunol Res. 2023;4(2):60-68. doi: 10.2478/rir-2023-0010
- Darakjian AA, Bhutani M, Fairweather D, et al. (2024) Similarities and differences in self-reported symptoms and comorbidities between hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorders. Rheumatol Adv Pract. 2024;8(4):rkae134. doi: 10.1093/rap/rkae134
- Petrucci T, Barclay SJ, Gensemer C, et al. (2024) Phenotypic Clusters and Multimorbidity in Hypermobile Ehlers-Danlos Syndrome. Mayo Clin Proc Innov Qual Outcomes. 2024;8(3):253-262. doi: 10.1016/j.mayocpiqo.2024.04.001
- Wu W, Ho V. (2024) An overview of Ehlers Danlos syndrome and the link between postural orthostatic tachycardia syndrome and gastrointestinal symptoms with a focus on gastroparesis. Front Neurol. 2024;15:1379646. doi: 10.3389/fneur.2024.1379646
- Tofts LJ, Simmonds J, Schwartz SB, et al. (2023) Pediatric joint hypermobility: a diagnostic framework and narrative review. Orphanet J Rare Dis. 2023;18(1):104. doi: 10.1186/s13023-023-02717-2
If you have seen claims about fascia being the missing piece in hypermobility, our deep dive on what the fascia research actually shows and what is being oversold is worth the read.